

Vaccine optimization for COVID-19: Who to vaccinate first?
- PMID: 33536223
- PMCID: PMC8128110
- DOI: 10.1126/sciadv.abf1374
Vaccine optimization for COVID-19: Who to vaccinate first?
Abstract
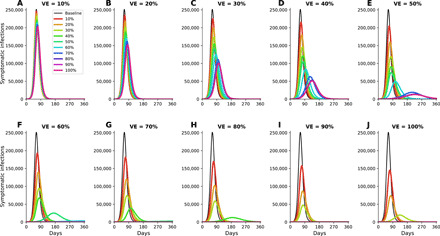
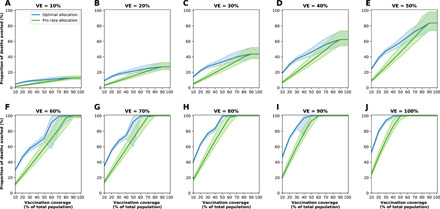
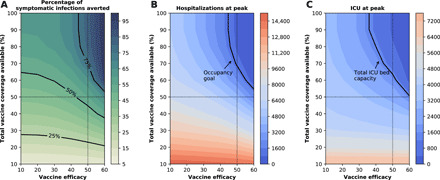
Vaccines, when available, will likely become our best tool to control the COVID-19 pandemic. Even in the most optimistic scenarios, vaccine shortages will likely occur. Using an age-stratified mathematical model paired with optimization algorithms, we determined optimal vaccine allocation for four different metrics (deaths, symptomatic infections, and maximum non-ICU and ICU hospitalizations) under many scenarios. We find that a vaccine with effectiveness ≥50% would be enough to substantially mitigate the ongoing pandemic, provided that a high percentage of the population is optimally vaccinated. When minimizing deaths, we find that for low vaccine effectiveness, irrespective of vaccination coverage, it is optimal to allocate vaccine to high-risk (older) age groups first. In contrast, for higher vaccine effectiveness, there is a switch to allocate vaccine to high-transmission (younger) age groups first for high vaccination coverage. While there are other societal and ethical considerations, this work can provide an evidence-based rationale for vaccine prioritization.
Copyright © 2021 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works. Distributed under a Creative Commons Attribution NonCommercial License 4.0 (CC BY-NC).
Figures







Update of
-
Vaccine optimization for COVID-19: who to vaccinate first?medRxiv [Preprint]. 2020 Dec 15:2020.08.14.20175257. doi: 10.1101/2020.08.14.20175257. medRxiv. 2020. Update in: Sci Adv. 2021 Feb 3;7(6):eabf1374. doi: 10.1126/sciadv.abf1374. PMID: 32817963 Free PMC article. Updated. Preprint.
References
-
- Johns Hopkins University and Medicine, Coronavirus COVID-19 global cases by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU) (2020); https://coronavirus.jhu.edu/map.html.
-
- C. Zimmer, J. Corum, S.-L. Wee, Coronavirus Vaccine Tracker (2020); https://www.nytimes.com/interactive/2020/science/coronavirus-vaccine-tra....
-
- Cohen R., Jung C., Ouldali N., Sellam A., Batard C., Cahn-Sellem F., Elbez A., Wollner A., Romain O., Corrard F., Aberrane S., Soismier N., Creidy R., Smati-Lafarge M., Launay O., Bechet S., Varon E., Levy C., Assessment of spread of SARS-CoV-2 by RT-PCR and concomitant serology in children in a region heavily affected by COVID-19 pandemic. medRxiv 2020.06.12.20129221 (2020).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
