

Tissue-Resident Memory T Cells in the Lungs Protect against Acute Respiratory Syncytial Virus Infection
- PMID: 33536235
- PMCID: PMC8299542
- DOI: 10.4049/immunohorizons.2000067
Tissue-Resident Memory T Cells in the Lungs Protect against Acute Respiratory Syncytial Virus Infection
Abstract
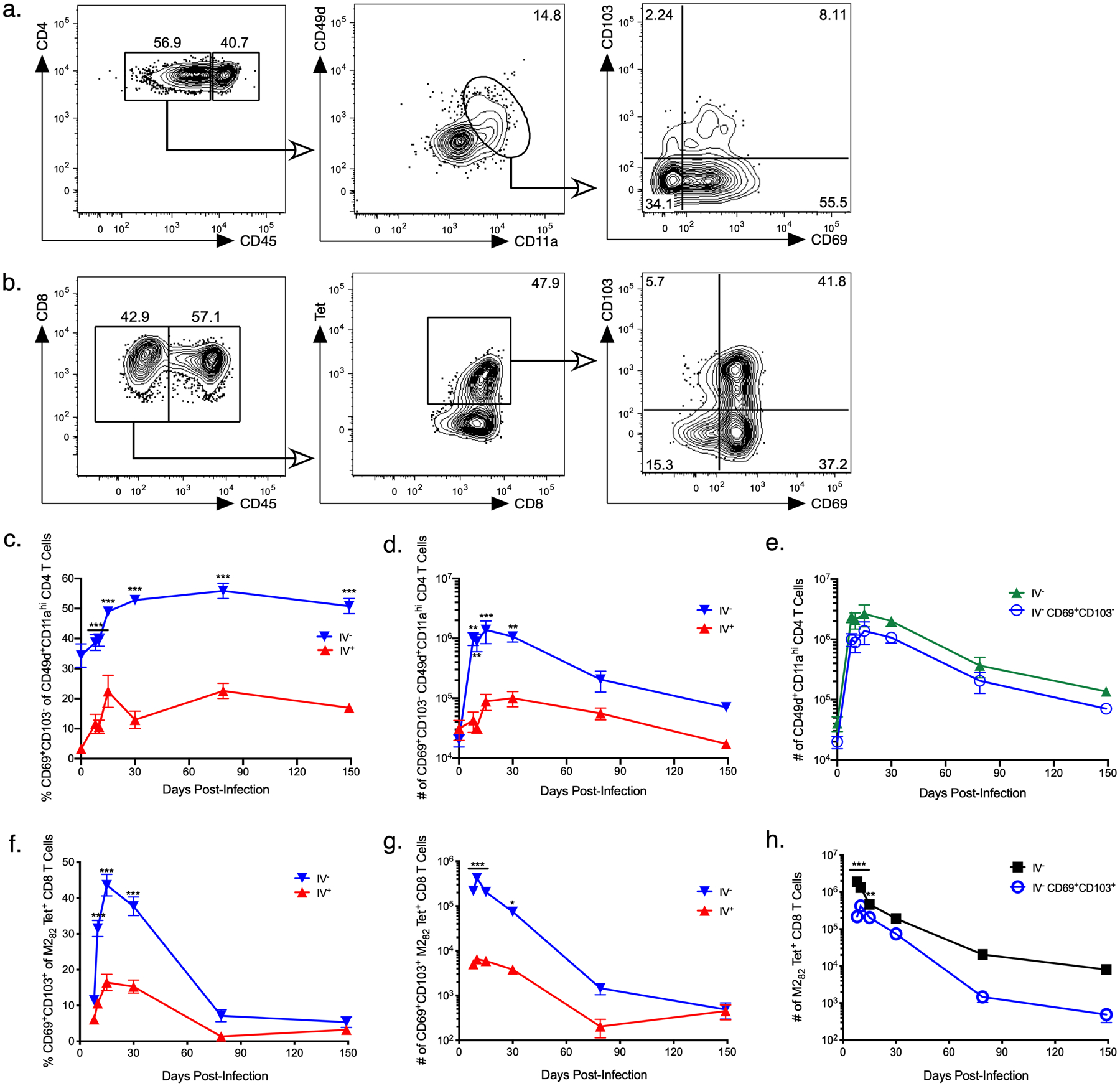
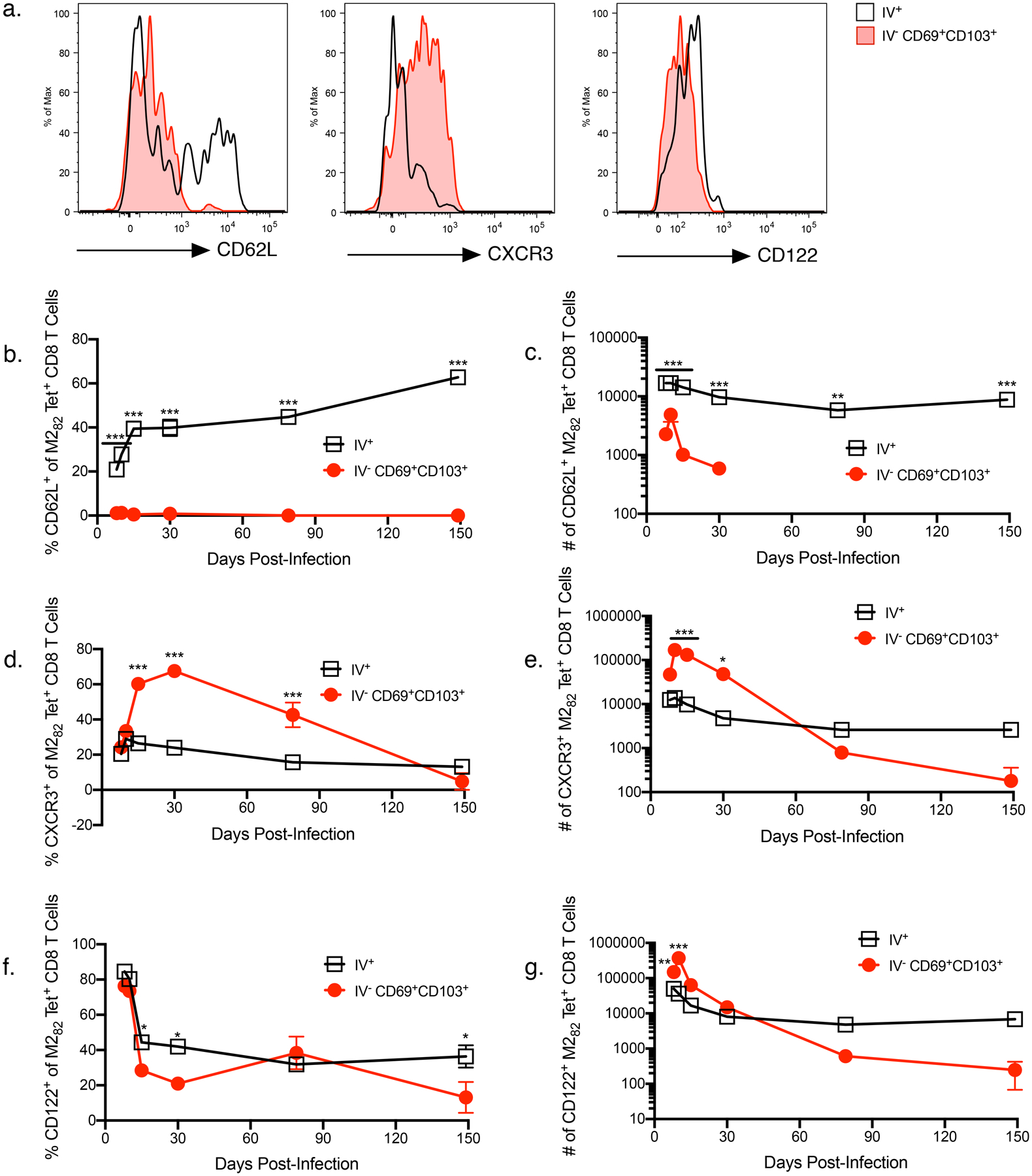
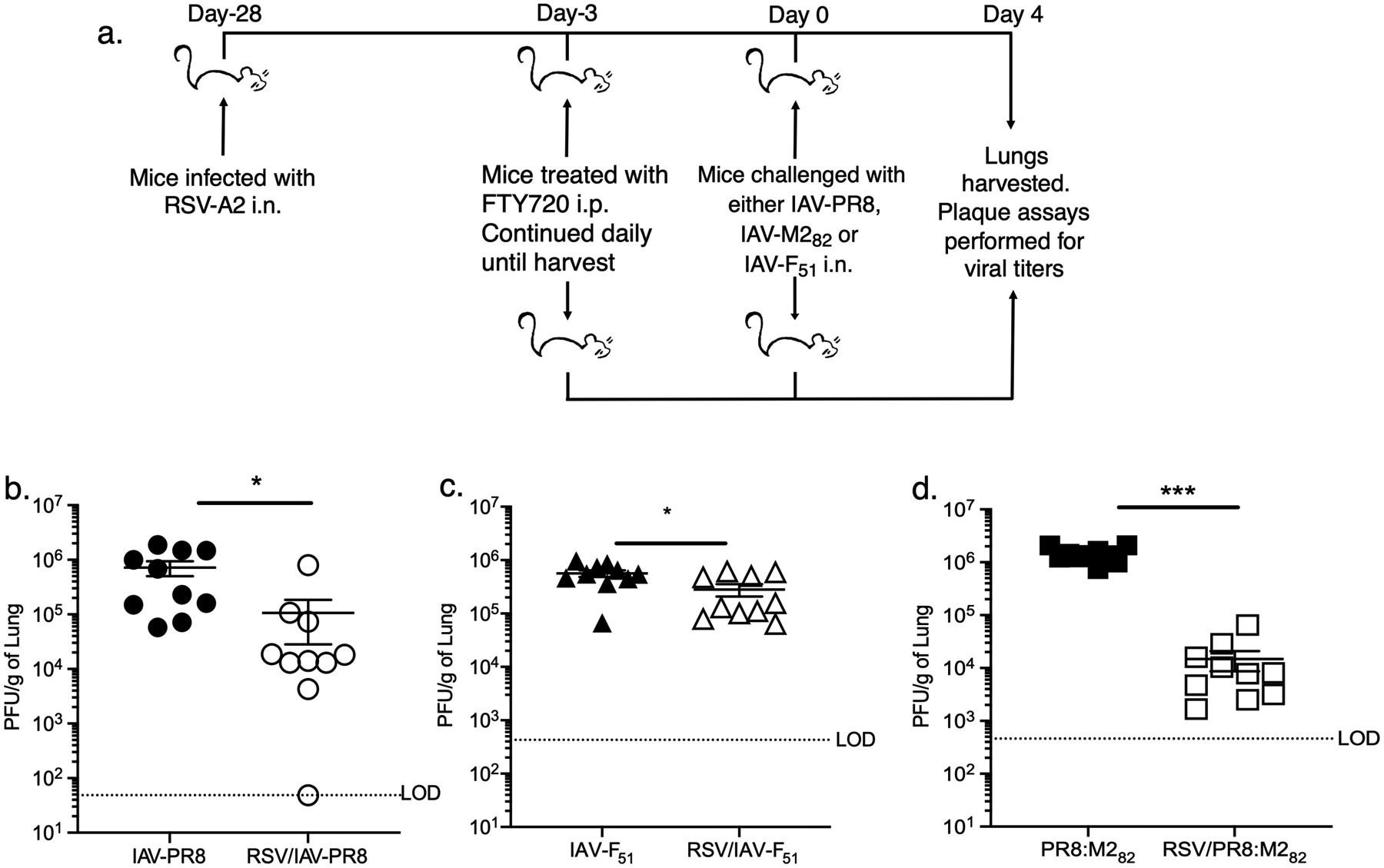
Respiratory syncytial virus (RSV) is the leading cause of lower respiratory tract infection in young children. The T cell response plays a critical role in facilitating clearance of an acute RSV infection, and memory T cell responses are vital for protection against secondary RSV exposures. Tissue-resident memory (TRM) T cells have been identified as a subset of memory T cells that reside in nonlymphoid tissues and are critical for providing long-term immunity. There is currently limited information regarding the establishment and longevity of TRM T cell responses elicited following an acute RSV infection as well as their role in protection against repeated RSV infections. In this study, we examined the magnitude, phenotype, and protective capacity of TRM CD4 and CD8 T cells in the lungs of BALB/c mice following an acute RSV infection. TRM CD4 and CD8 T cells were established within the lungs and waned by 149 d following RSV infection. To determine the protective capacity of TRMs, FTY720 administration was used to prevent trafficking of peripheral memory T cells into the lungs prior to challenge of RSV-immune mice, with a recombinant influenza virus expressing either an RSV-derived CD4 or CD8 T cell epitope. We observed enhanced viral clearance in RSV-immune mice, suggesting that TRM CD8 T cells can contribute to protection against a secondary RSV infection. Given the protective capacity of TRMs, future RSV vaccine candidates should focus on the generation of these cell populations within the lung to induce effective immunity against RSV infection.
Copyright © 2021 The Authors.
Figures


Similar articles
-
Conserved T-cell epitopes of respiratory syncytial virus (RSV) delivered by recombinant live attenuated influenza vaccine viruses efficiently induce RSV-specific lung-localized memory T cells and augment influenza-specific resident memory T-cell responses.Antiviral Res. 2020 Oct;182:104864. doi: 10.1016/j.antiviral.2020.104864. Epub 2020 Jun 22. Antiviral Res. 2020. PMID: 32585323 Free PMC article.
-
Type I interferons and MAVS signaling are necessary for tissue resident memory CD8+ T cell responses to RSV infection.PLoS Pathog. 2022 Feb 2;18(2):e1010272. doi: 10.1371/journal.ppat.1010272. eCollection 2022 Feb. PLoS Pathog. 2022. PMID: 35108347 Free PMC article.
-
The number of respiratory syncytial virus (RSV)-specific memory CD8 T cells in the lung is critical for their ability to inhibit RSV vaccine-enhanced pulmonary eosinophilia.J Immunol. 2008 Dec 1;181(11):7958-68. doi: 10.4049/jimmunol.181.11.7958. J Immunol. 2008. PMID: 19017987 Free PMC article.
-
Induction and Subversion of Human Protective Immunity: Contrasting Influenza and Respiratory Syncytial Virus.Front Immunol. 2018 Mar 2;9:323. doi: 10.3389/fimmu.2018.00323. eCollection 2018. Front Immunol. 2018. PMID: 29552008 Free PMC article. Review.
-
CD8+ T cell immunity against human respiratory syncytial virus.Vaccine. 2014 Oct 21;32(46):6130-7. doi: 10.1016/j.vaccine.2014.08.063. Epub 2014 Sep 16. Vaccine. 2014. PMID: 25223272 Review.
Cited by
-
Vaccine-induced systemic and mucosal T cell immunity to SARS-CoV-2 viral variants.Proc Natl Acad Sci U S A. 2022 May 17;119(20):e2118312119. doi: 10.1073/pnas.2118312119. Epub 2022 May 13. Proc Natl Acad Sci U S A. 2022. PMID: 35561224 Free PMC article.
-
The Roles of Tissue-Resident Memory T Cells in Lung Diseases.Front Immunol. 2021 Oct 11;12:710375. doi: 10.3389/fimmu.2021.710375. eCollection 2021. Front Immunol. 2021. PMID: 34707601 Free PMC article. Review.
-
Modulating cytokine microenvironment during T cell activation induces protective RSV-specific lung resident memory T cells in early life in mice.Npj Viruses. 2024 Dec 31;2(1):71. doi: 10.1038/s44298-024-00073-x. eCollection 2024 Dec. Npj Viruses. 2024. PMID: 39749186 Free PMC article.
-
Memory T Cells in Respiratory Virus Infections: Protective Potential and Persistent Vulnerabilities.Med Sci (Basel). 2025 Apr 29;13(2):48. doi: 10.3390/medsci13020048. Med Sci (Basel). 2025. PMID: 40407543 Free PMC article. Review.
-
T cell immune memory after covid-19 and vaccination.BMJ Med. 2023 Nov 22;2(1):e000468. doi: 10.1136/bmjmed-2022-000468. eCollection 2023. BMJ Med. 2023. PMID: 38027416 Free PMC article. Review.
References
-
- Shi T, McAllister DA, O’Brien KL, Simoes EAF, Madhi SA, Gessner BD, Polack FP, Balsells E, Acacio S, Aguayo C, Alassani I, Ali A, Antonio M, Awasthi S, Awori JO, Azziz-Baumgartner E, Baggett HC, Baillie VL, Balmaseda A, Barahona A, Basnet S, Bassat Q, Basualdo W, Bigogo G, Bont L, Breiman RF, Brooks WA, Broor S, Bruce N, Bruden D, Buchy P, Campbell S, Carosone-Link P, Chadha M, Chipeta J, Chou M, Clara W, Cohen C, de Cuellar E, Dang DA, Dash-Yandag B, Deloria-Knoll M, Dherani M, Eap T, Ebruke BE, Echavarria M, de Freitas Lazaro Emediato CC, Fasce RA, Feikin DR, Feng L, Gentile A, Gordon A, Goswami D, Goyet S, Groome M, Halasa N, Hirve S, Homaira N, Howie SRC, Jara J, Jroundi I, Kartasasmita CB, Khuri-Bulos N, Kotloff KL, Krishnan A, Libster R, Lopez O, Lucero MG, Lucion F, Lupisan SP, Marcone DN, McCracken JP, Mejia M, Moisi JC, Montgomery JM, Moore DP, Moraleda C, Moyes J, Munywoki P, Mutyara K, Nicol MP, Nokes DJ, Nymadawa P, da Costa Oliveira MT, Oshitani H, Pandey N, Paranhos-Baccala G, Phillips LN, Picot VS, Rahman M, Rakoto-Andrianarivelo M, Rasmussen ZA, Rath BA, Robinson A, Romero C, Russomando G, Salimi V, Sawatwong P, Scheltema N, Schweiger B, Scott JAG, Seidenberg P, Shen K, Singleton R, Sotomayor V, Strand TA, Sutanto A, Sylla M, Tapia MD, Thamthitiwat S, Thomas ED, Tokarz R, Turner C, Venter M, Waicharoen S, Wang J, Watthanaworawit W, Yoshida LM, Yu H, Zar HJ, Campbell H, and Nair H. 2017. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet. 390: 946–958. - PMC - PubMed
-
- Glezen WP, Taber LH, Frank AL, and Kasel JA. 1986. Risk of primary infection and reinfection with respiratory syncytial virus. Am. J. Dis. Child 140: 543–546. - PubMed
-
- Kim HW, Canchola JG, Brandt CD, Pyles G, Chanock RM, Jensen K, and Parrott RH. 1969. Respiratory Syncytial Virus Disease in Infants Despite Prior Administration of Antigenic Inactivated Vaccine. Am. J. Epidemiol 89: 422–434. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
