

Precision medicine in acute respiratory distress syndrome: workshop report and recommendations for future research
- PMID: 33536264
- PMCID: PMC8522998
- DOI: 10.1183/16000617.0317-2020
Precision medicine in acute respiratory distress syndrome: workshop report and recommendations for future research
Abstract
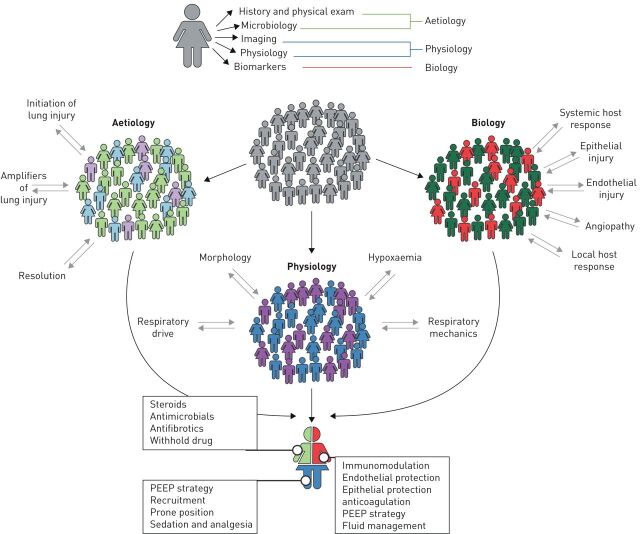
Acute respiratory distress syndrome (ARDS) is a devastating critical illness that can be triggered by a wide range of insults and remains associated with a high mortality of around 40%. The search for targeted treatment for ARDS has been disappointing, possibly due to the enormous heterogeneity within the syndrome. In this perspective from the European Respiratory Society research seminar on "Precision medicine in ARDS", we will summarise the current evidence for heterogeneity, explore the evidence in favour of precision medicine and provide a roadmap for further research in ARDS. There is evident variation in the presentation of ARDS on three distinct levels: 1) aetiological; 2) physiological and 3) biological, which leads us to the conclusion that there is no typical ARDS. The lack of a common presentation implies that intervention studies in patients with ARDS need to be phenotype aware and apply a precision medicine approach in order to avoid the lack of success in therapeutic trials that we faced in recent decades. Deeper phenotyping and integrative analysis of the sources of variation might result in identification of additional treatable traits that represent specific pathobiological mechanisms, or so-called endotypes.
Copyright ©ERS 2021.
Conflict of interest statement
Conflict of interest: L.D.J. Bos reports grants from the Dutch Lung Foundation (Young investigator grant), the Dutch Lung Foundation and Health Holland (Public–Private Partnership grant) and the Dutch Lung Foundation (Dirkje Postma Award), and grants from IMI COVID19 imitative and Amsterdam UMC Fellowship, outside the submitted work. Conflict of interest: A. Artigas reports grants from Grifols and Fisher & Paykel, and personal fees from Grifols, outside the submitted work. Conflict of interest: J-M. Constantin has nothing to disclose. Conflict of interest: L.A. Hagens has nothing to disclose. Conflict of interest: N. Heijnen has nothing to disclose. Conflict of interest: J.G. Laffey reports grants from Science Foundation Ireland and Health Research Board Ireland, outside the submitted work. Conflict of interest: N. Meyer reports grants from National Institutes of Health, outside the submitted work. Conflict of interest: L. Papazian has nothing to disclose. Conflict of interest: L. Pisani reports personal fees from Fisher & Paykel, outside the submitted work. Conflict of interest: M.J. Schultz has nothing to disclose. Conflict of interest: M. Shankar-Hari has nothing to disclose. Conflict of interest: M.R. Smit has nothing to disclose. Conflict of interest: C. Summers reports grants from GlaxoSmithKline and AstraZeneca, outside the submitted work. Conflict of interest: L.B. Ware reports grants from National Institutes of Health, during the conduct of the study; other funding from CSL Behring, Genentech and Global Blood Therapeutics, and personal fees from Merck, Bayer and Quark, outside the submitted work. Conflict of interest: R. Scala has nothing to disclose. Conflict of interest: C. Calfee reports grants from NIH, during the conduct of the study; grants and personal fees from Roche/Genentech and Bayer, personal fees from Quark Pharmaceuticals, Prometic, Gen1e Life Sciences and Vasomune, outside the submitted work.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources