

Data-driven identification of ageing-related diseases from electronic health records
- PMID: 33536532
- PMCID: PMC7859412
- DOI: 10.1038/s41598-021-82459-y
Data-driven identification of ageing-related diseases from electronic health records
Abstract
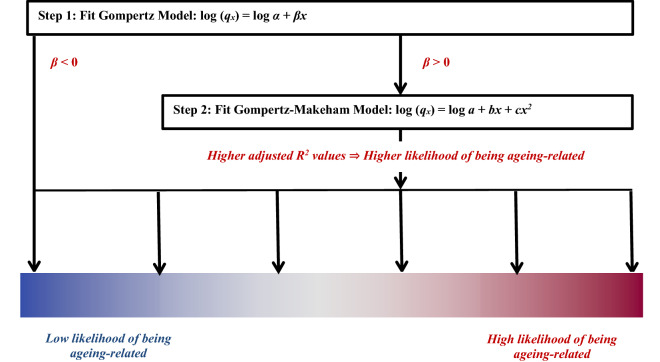
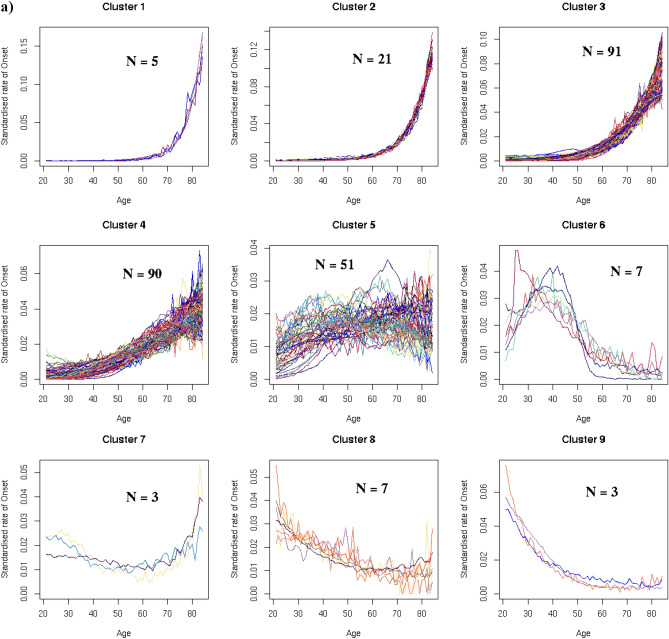
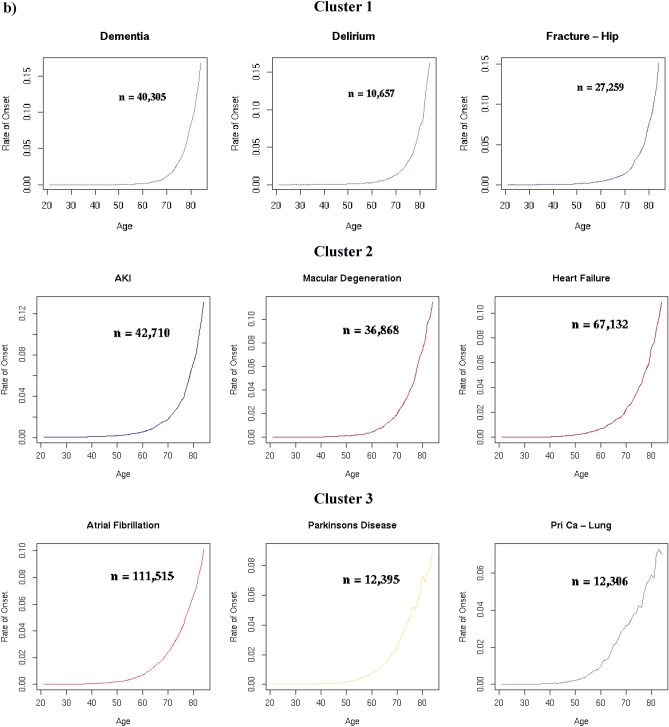
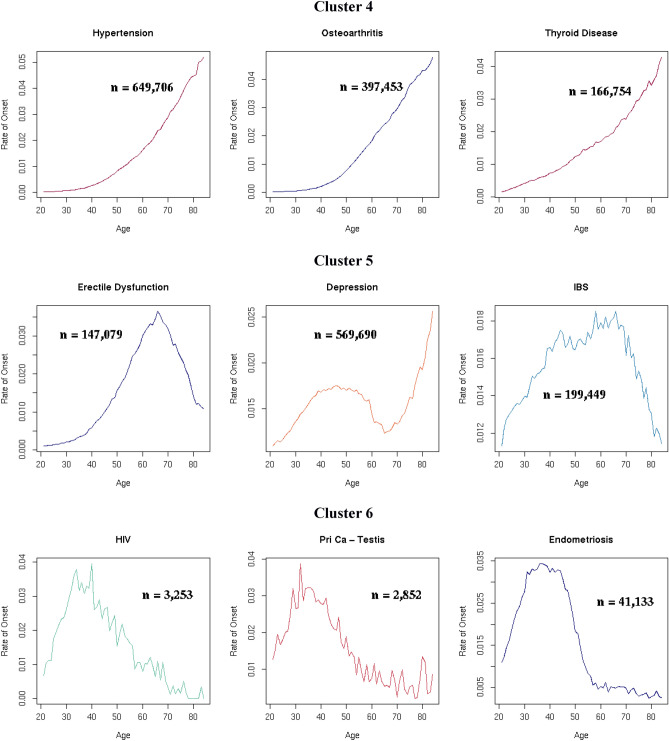
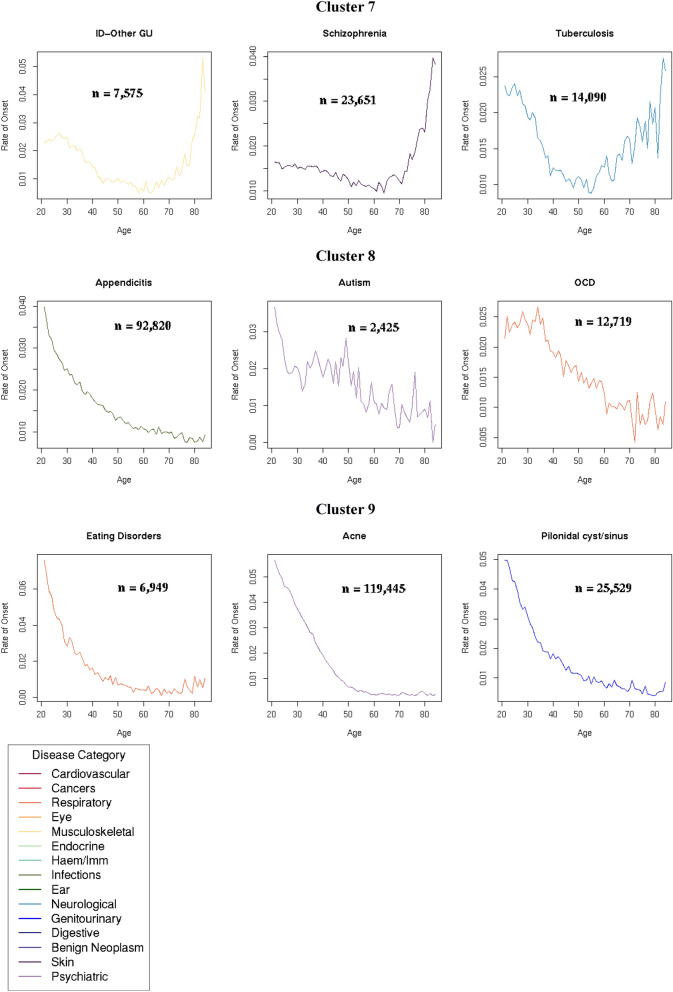
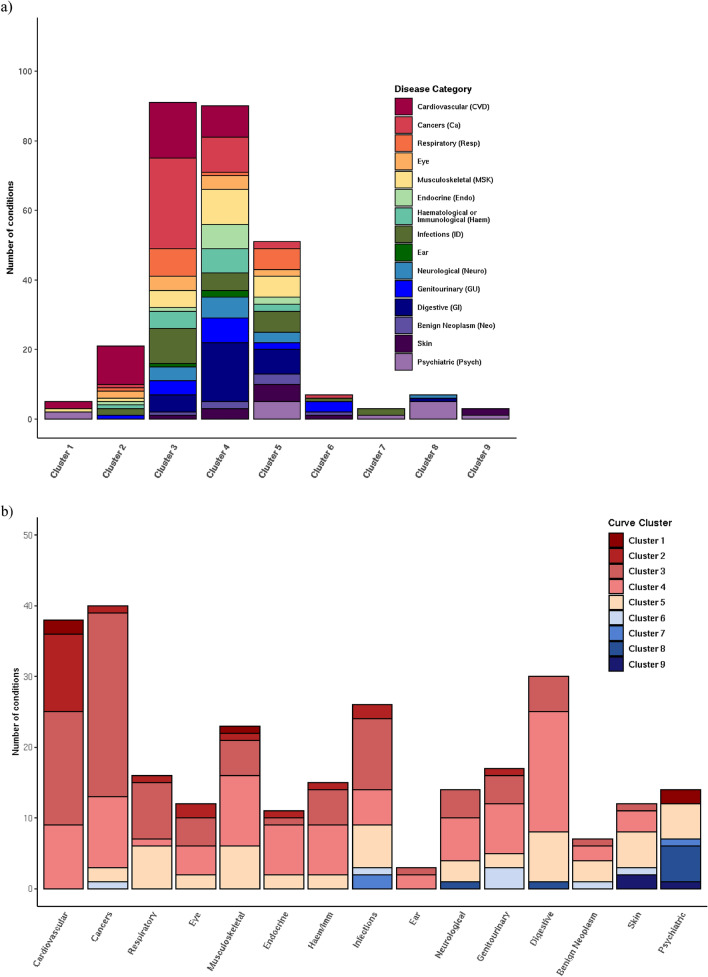
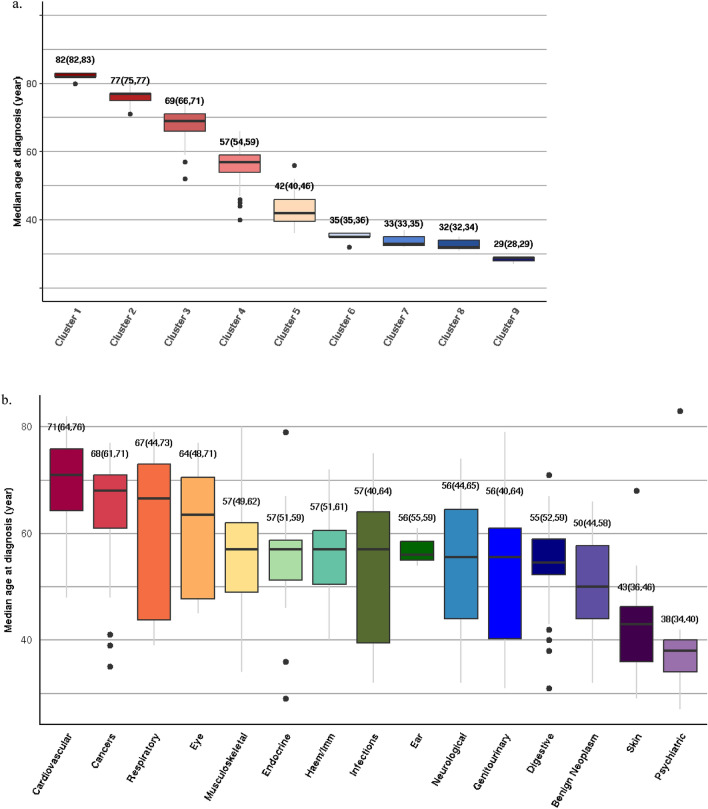
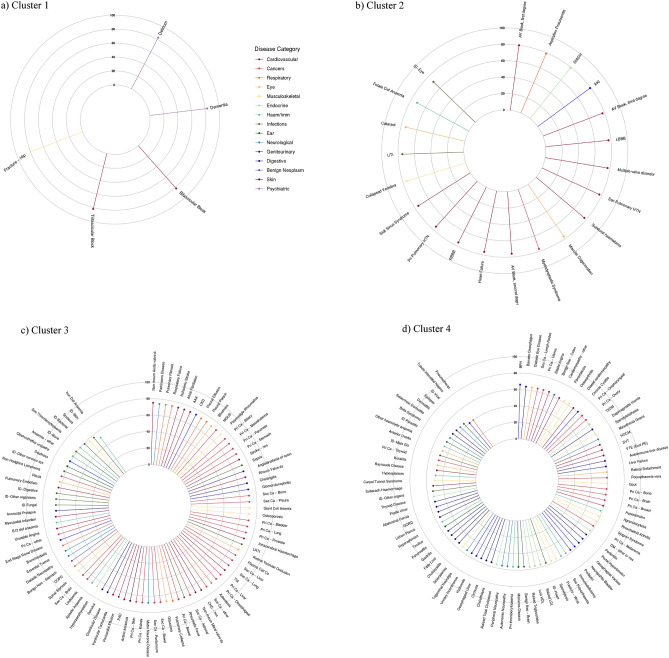
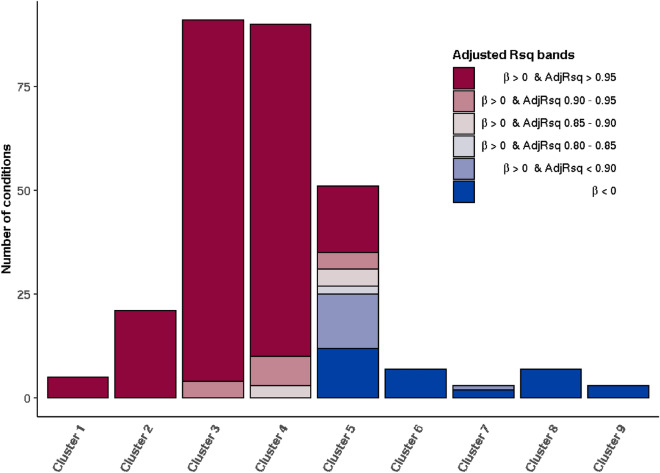
Reducing the burden of late-life morbidity requires an understanding of the mechanisms of ageing-related diseases (ARDs), defined as diseases that accumulate with increasing age. This has been hampered by the lack of formal criteria to identify ARDs. Here, we present a framework to identify ARDs using two complementary methods consisting of unsupervised machine learning and actuarial techniques, which we applied to electronic health records (EHRs) from 3,009,048 individuals in England using primary care data from the Clinical Practice Research Datalink (CPRD) linked to the Hospital Episode Statistics admitted patient care dataset between 1 April 2010 and 31 March 2015 (mean age 49.7 years (s.d. 18.6), 51% female, 70% white ethnicity). We grouped 278 high-burden diseases into nine main clusters according to their patterns of disease onset, using a hierarchical agglomerative clustering algorithm. Four of these clusters, encompassing 207 diseases spanning diverse organ systems and clinical specialties, had rates of disease onset that clearly increased with chronological age. However, the ages of onset for these four clusters were strikingly different, with median age of onset 82 years (IQR 82-83) for Cluster 1, 77 years (IQR 75-77) for Cluster 2, 69 years (IQR 66-71) for Cluster 3 and 57 years (IQR 54-59) for Cluster 4. Fitting to ageing-related actuarial models confirmed that the vast majority of these 207 diseases had a high probability of being ageing-related. Cardiovascular diseases and cancers were highly represented, while benign neoplastic, skin and psychiatric conditions were largely absent from the four ageing-related clusters. Our framework identifies and clusters ARDs and can form the basis for fundamental and translational research into ageing pathways.
Conflict of interest statement
DN is on the steering group for grants funded by Glaxo Smith Kline and her team was subcontracted by Informatica to carry out the analyses of the National CKD Audit. RTL reports grants from Pfizer. ICKW is a member of the Independent Scientific Advisory Committee (ISAC) of Clinical Practice Research Datalink (CPRD). VK, HCF, MH, SD, AGI, KD, RM, CAP, RS, JPC, JMT, HH, LP and ADH declare no potential competing interest.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
