

Comparison of Mortality Risk Models in Patients with Postcardiac Arrest Cardiogenic Shock and Percutaneous Mechanical Circulatory Support
- PMID: 33536855
- PMCID: PMC7834787
- DOI: 10.1155/2021/8843935
Comparison of Mortality Risk Models in Patients with Postcardiac Arrest Cardiogenic Shock and Percutaneous Mechanical Circulatory Support
Abstract
Background: Although scoring systems are widely used to predict outcomes in postcardiac arrest cardiogenic shock (CS) after out-of-hospital cardiac arrest (OHCA) complicating acute myocardial infarction (AMI), data concerning the accuracy of these scores to predict mortality of patients treated with Impella in this setting are lacking. Thus, we aimed to evaluate as well as to compare the prognostic accuracy of acute physiology and chronic health II (APACHE II), simplified acute physiology score II (SAPS II), sepsis-related organ failure assessment (SOFA), the intra-aortic balloon pump (IABP), CardShock, the prediction of cardiogenic shock outcome for AMI patients salvaged by VA-ECMO (ENCOURAGE), and the survival after venoarterial extracorporeal membrane oxygenation (SAVE) score in patients with OHCA refractory CS due to an AMI treated with Impella 2.5 or CP.
Methods: Retrospective study of 65 consecutive Impella 2.5 and 32 CP patients treated in our cardiac arrest center from September 2015 until June 2020.
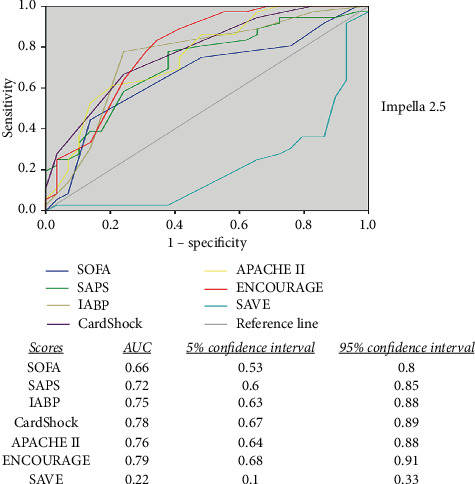
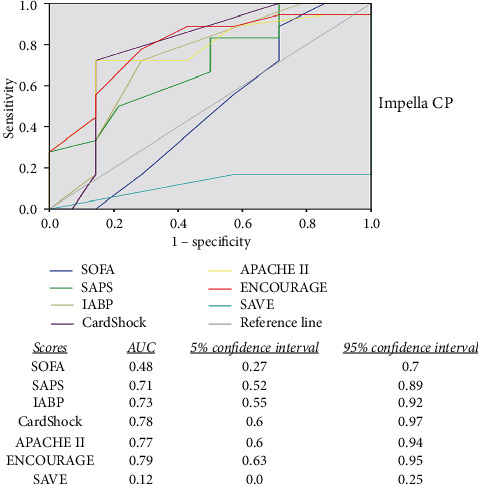
Results: Overall survival to discharge was 44.3%. The expected mortality according to scores was SOFA 70%, SAPS II 90%, IABP shock 55%, CardShock 80%, APACHE II 85%, ENCOURAGE 50%, and SAVE score 70% in the 2.5 group; SOFA 70%, SAPS II 85%, IABP shock 55%, CardShock 80%, APACHE II 85%, ENCOURAGE 75%, and SAVE score 70% in the CP group. The ENCOURAGE score was the most effective predictive model of mortality outcome presenting a moderate area under the curve (AUC) of 0.79, followed by the CardShock, APACHE II, IABP, and SAPS score. These derived an AUC between 0.71 and 0.78. The SOFA and the SAVE scores failed to predict the outcome in this particular setting of refractory CS after OHCA due to an AMI.
Conclusion: The available intensive care and newly developed CS scores offered only a moderate prognostic accuracy for outcomes in OHCA patients with refractory CS due to an AMI treated with Impella. A new score is needed in order to guide the therapy in these patients.
Copyright © 2021 Georgios Chatzis et al.
Conflict of interest statement
Drs. Schieffer, Karatolios, Markus, and Luesebrink have received speaker's honoraria from Abiomed. Drs. Chatzis, Syntila, Divchev, Ahrens, and Waechter declare no conflicts of interest.
Figures
Similar articles
-
Value of APACHE II, SOFA and CardShock scoring as predictive tools for cardiogenic shock: A single-centre pilot study.ESC Heart Fail. 2024 Dec;11(6):3584-3597. doi: 10.1002/ehf2.15020. Epub 2024 Aug 13. ESC Heart Fail. 2024. PMID: 39136422 Free PMC article.
-
Trends in mechanical circulatory support use and hospital mortality among patients with acute myocardial infarction and non-infarction related cardiogenic shock in the United States.Clin Res Cardiol. 2018 Apr;107(4):287-303. doi: 10.1007/s00392-017-1182-2. Epub 2017 Nov 13. Clin Res Cardiol. 2018. PMID: 29134345
-
Predictive value of outcome scores in patients suffering from cardiogenic shock complicating AMI: APACHE II, APACHE III, Elebute-Stoner, SOFA, and SAPS II.Med Klin Intensivmed Notfmed. 2013 Nov;108(8):666-74. doi: 10.1007/s00063-013-0234-2. Epub 2013 Apr 6. Med Klin Intensivmed Notfmed. 2013. PMID: 23558639
-
Concomitant Intra-Aortic Balloon Pump Use in Cardiogenic Shock Requiring Veno-Arterial Extracorporeal Membrane Oxygenation.Circ Cardiovasc Interv. 2018 Sep;11(9):e006930. doi: 10.1161/CIRCINTERVENTIONS.118.006930. Circ Cardiovasc Interv. 2018. PMID: 30354593
-
Mortality in cardiogenic shock patients receiving mechanical circulatory support: a network meta-analysis.BMC Cardiovasc Disord. 2022 Feb 13;22(1):48. doi: 10.1186/s12872-022-02493-0. BMC Cardiovasc Disord. 2022. PMID: 35152887 Free PMC article.
Cited by
-
Comparison of Risk Models in the Prediction of 30-Day Mortality in Acute Myocardial Infarction-Associated Cardiogenic Shock.Struct Heart. 2022 Oct 31;6(6):100116. doi: 10.1016/j.shj.2022.100116. eCollection 2022 Nov. Struct Heart. 2022. PMID: 37288128 Free PMC article.
-
Predicting survival after Impella implantation in patients with cardiogenic shock: The J-PVAD risk score.Eur J Heart Fail. 2025 Jan;27(1):51-59. doi: 10.1002/ejhf.3471. Epub 2024 Sep 19. Eur J Heart Fail. 2025. PMID: 39300761 Free PMC article.
-
Lactate versus Phosphate as Biomarkers to Aid Mechanical Circulatory Support Decisions in Patients with Out-of-Hospital Cardiac Arrest and Return of Spontaneous Circulation.Diagnostics (Basel). 2023 Apr 24;13(9):1523. doi: 10.3390/diagnostics13091523. Diagnostics (Basel). 2023. PMID: 37174915 Free PMC article.
References
-
- Hochman J. S., Buller C. E., Sleeper L. A., et al. Cardiogenic shock complicating acute myocardial infarction--etiologies, management and outcome: a report from the SHOCK trial registry should we emergently revascularize occluded coronaries for cardiogenic shock? Journal of the American College of Cardiology. 2000;36(3):1063–1070. doi: 10.1016/s0735-1097(00)00879-2. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
