

Japanese Practice Guidelines for Fecal Incontinence Part 3 -Surgical Treatment for Fecal Incontinence, Fecal Incontinence in a Special Conditions- English Version
- PMID: 33537503
- PMCID: PMC7843139
- DOI: 10.23922/jarc.2020-075
Japanese Practice Guidelines for Fecal Incontinence Part 3 -Surgical Treatment for Fecal Incontinence, Fecal Incontinence in a Special Conditions- English Version
Abstract
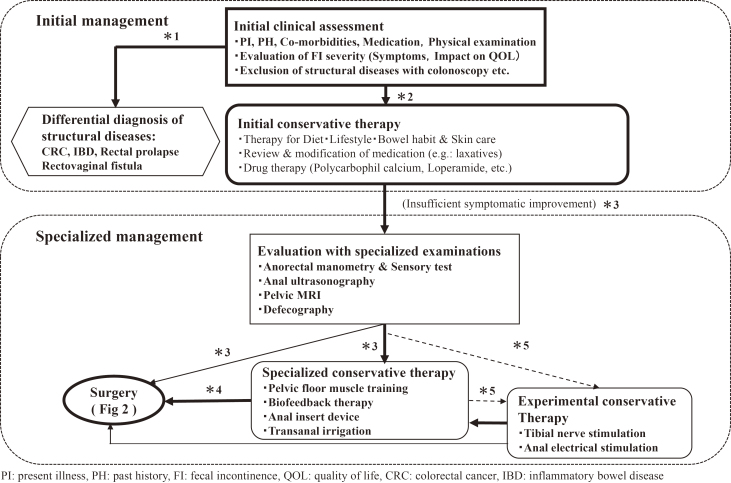
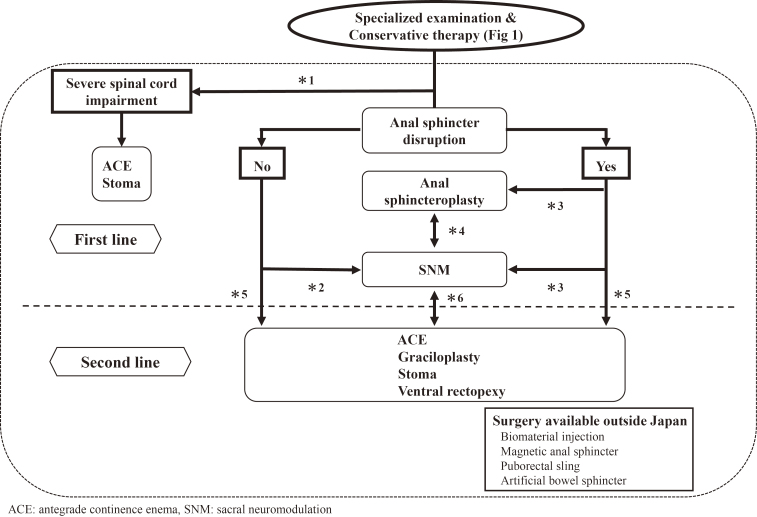
In Japan, the surgical treatment for fecal incontinence (FI) can be performed using minimally invasive surgery, such as anal sphincteroplasty and sacral neuromodulation (SNM), as well as antegrade continence enema (ACE), graciloplasty, and stoma construction. In addition, currently, several other procedures, including biomaterial injection therapy, artificial bowel sphincter (ABS), and magnetic anal sphincter (MAS), are unavailable in Japan but are performed in Western countries. The evidence level of surgical treatment for FI is generally low, except for novel procedures, such as SNM, which was covered by health insurance in Japan since 2014. Although the surgical treatment algorithm for FI has been chronologically modified, it should be sequentially selected, starting from the most minimally invasive procedure, as FI is a benign condition. Injuries to the neural system or spinal cord often cause disorders of the sensory and motor nerves that innervate the anus, rectum, and pelvic floor, leading to the difficulty in controlling bowel movement or FI and/or constipation. FI and constipation are closely associated; when one improves, the other tends to deteriorate. Patients with severe cognitive impairment may present with active soiling, referred to as "incontinence" episodes that occur as a consequence of abnormal behavior, and may also experience passive soiling.
Keywords: Japanese guidelines; defecation disorders; fecal incontinence; fecal incontinence in a special condition; practice guideline; surgical treatments.
Copyright © 2021 by The Japan Society of Coloproctology.
Conflict of interest statement
Conflicts of Interest There are no conflicts of interest.
Figures
Similar articles
-
Surgical Interventions and the Use of Device-Aided Therapy for the Treatment of Fecal Incontinence and Defecatory Disorders.Clin Gastroenterol Hepatol. 2017 Dec;15(12):1844-1854. doi: 10.1016/j.cgh.2017.08.023. Epub 2017 Aug 22. Clin Gastroenterol Hepatol. 2017. PMID: 28838787 Free PMC article. Review.
-
Japanese Practice Guidelines for Fecal Incontinence Part 2-Examination and Conservative Treatment for Fecal Incontinence- English Version.J Anus Rectum Colon. 2021 Jan 28;5(1):67-83. doi: 10.23922/jarc.2020-079. eCollection 2021. J Anus Rectum Colon. 2021. PMID: 33537502 Free PMC article. Review.
-
Comparison of antegrade continence enema treatment and sacral nerve stimulation for children with severe functional constipation and fecal incontinence.Neurogastroenterol Motil. 2020 Aug;32(8):e13809. doi: 10.1111/nmo.13809. Epub 2020 Feb 3. Neurogastroenterol Motil. 2020. PMID: 32017325 Free PMC article.
-
The relationship between fecal incontinence, constipation and defecatory symptoms in women with pelvic floor disorders.Neurourol Urodyn. 2017 Feb;36(2):495-498. doi: 10.1002/nau.22964. Epub 2016 Feb 1. Neurourol Urodyn. 2017. PMID: 26828646
-
Fecal incontinence. Studies on physiology, pathophysiology and surgical treatment.Dan Med Bull. 2003 Aug;50(3):262-82. Dan Med Bull. 2003. PMID: 13677243 Review.
Cited by
-
An Exploratory Study on the Contractile Effects of Hydroxy-α-Sanshool and Hydroxy-β-Sanshool, the Active Ingredients of Daikenchuto, on the Internal Anal Sphincter.J Anus Rectum Colon. 2023 Jul 25;7(3):206-213. doi: 10.23922/jarc.2023-001. eCollection 2023. J Anus Rectum Colon. 2023. PMID: 37496571 Free PMC article.
-
Injection of aluminum potassium sulfate and tannic acid in the treatment of fecal incontinence: a single-center observational study.Ann Coloproctol. 2022 Dec;38(6):403-408. doi: 10.3393/ac.2021.00248.0035. Epub 2021 Jul 21. Ann Coloproctol. 2022. PMID: 34284557 Free PMC article.
-
Fecal Incontinence: The Importance of a Structured Pathophysiological Model.J Anus Rectum Colon. 2022 Jan 28;6(1):58-66. doi: 10.23922/jarc.2021-040. eCollection 2022. J Anus Rectum Colon. 2022. PMID: 35128138 Free PMC article. Review.
-
The Role of Graciloplasty in the Treatment of Obstetric Anal Sphincter Injury with Subsequent Fecal Incontinence and Recurrent Low Recto-Vaginal Fistula: A Case Report.Reports (MDPI). 2025 Jan 20;8(1):11. doi: 10.3390/reports8010011. Reports (MDPI). 2025. PMID: 40729224 Free PMC article.
References
-
- Maeda K, Yamana T, Takao Y, et al. Japanese practice guidelines for fecal incontinence part 1 -Definition, epidemiology, etiology, pathophysiology and causes, risk factors, clinical evaluations, and symptomatic scores and QoL questionnaire for clinical evaluations- english Version. J Anus Rectum Colon. 2021 Jan; 5(1): 52-66. - PMC - PubMed
-
- Tjandra JJ, Han WR, Goh J, et al. Direct repair vs. overlapping sphincter repair: a randomized, controlled trial. Dis Colon Rectum. 2003 Jul; 46(7): 937-42; discussion 42-3. - PubMed
-
- Madoff RD, Parker SC, Varma MG, et al. Faecal incontinence in adults. Lancet. 2004 Aug: 364(9434): 621-32. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous