

Long-Term Antithrombotic Therapy and Clinical Outcomes in Patients with Acute Coronary Syndrome and Renal Impairment: Insights from EPICOR and EPICOR Asia
- PMID: 33537947
- PMCID: PMC8263456
- DOI: 10.1007/s40256-020-00447-5
Long-Term Antithrombotic Therapy and Clinical Outcomes in Patients with Acute Coronary Syndrome and Renal Impairment: Insights from EPICOR and EPICOR Asia
Abstract
Background: Information is lacking on long-term management of patients with acute coronary syndrome (ACS) and chronic kidney disease (CKD) (estimated glomerular filtration rate [eGFR] < 60 mL/min/1.73 m2).
Objectives: Our objectives were to describe antithrombotic management patterns and outcomes in patients with ACS with varying renal function from the EPICOR (long-tErm follow-uP of antithrombotic management patterns In acute CORonary syndrome patients; NCT01171404) and EPICOR Asia (NCT01361386) studies.
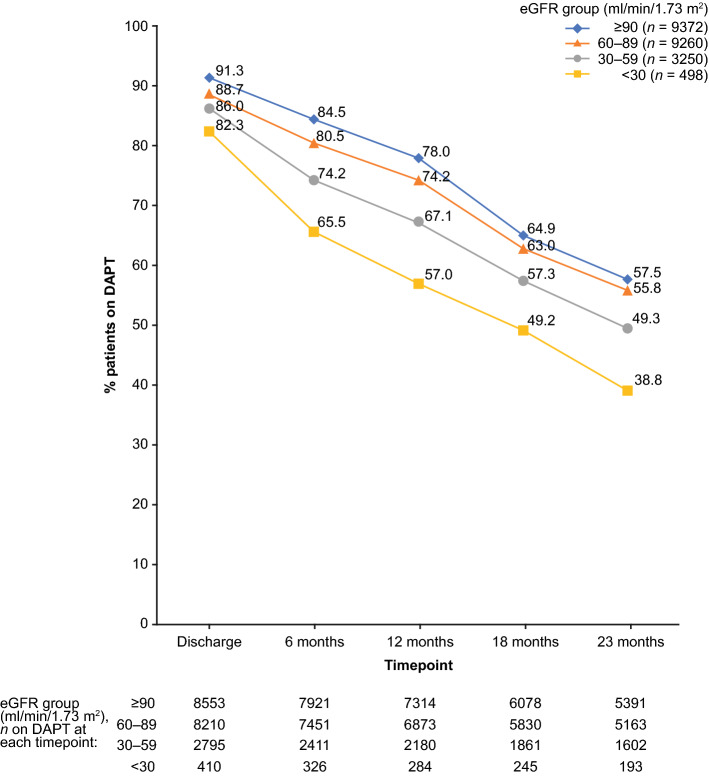
Methods: EPICOR and EPICOR Asia were prospective observational studies of patients who survived hospitalization for ACS and were enrolled at discharge in 28 countries across Europe, Latin America, and Asia. The studies were conducted from 2010 to 2013 and from 2011 to 2014, respectively. This analysis evaluated patient characteristics and oral antithrombotic management patterns and outcomes up to 2 years post-discharge according to admission eGFR: ≥ 90, 60-89, 30-59, or < 30 mL/min/1.73 m2.
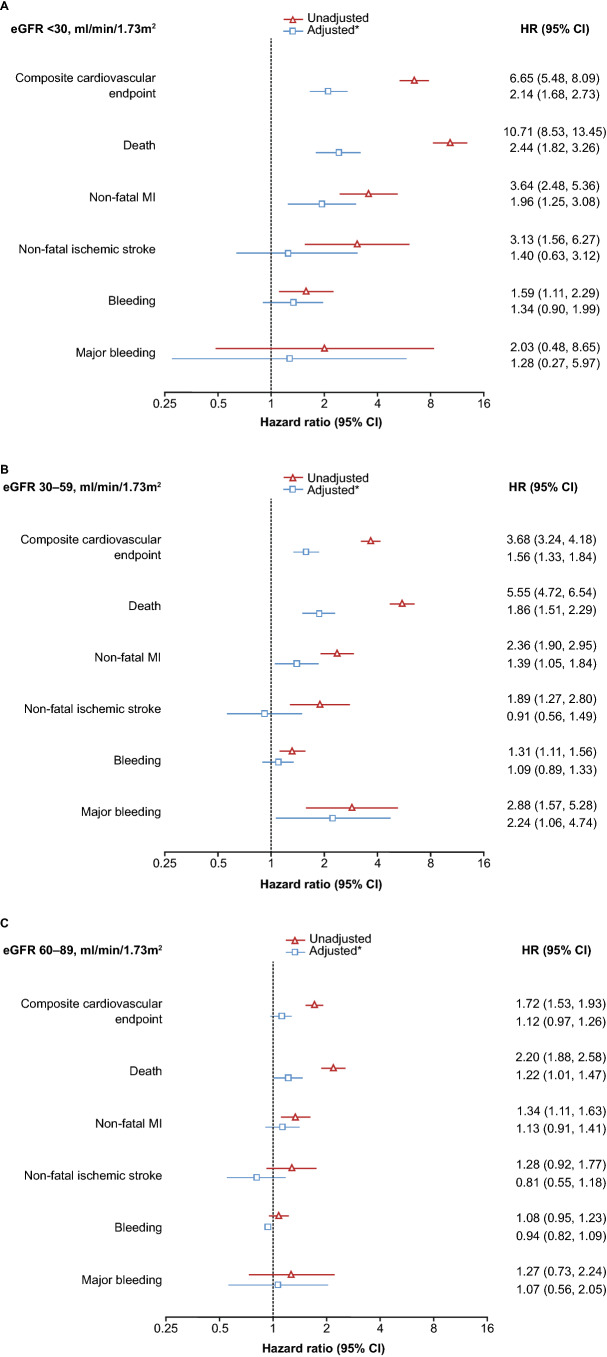
Results: Among 22,380 patients with available data, eGFR < 60 mL/min/1.73 m2 was observed in 16.7%. Patients with poorer renal function were older, were at greater cardiovascular risk, and had more prior cardiovascular disease and bleeding. Patients with CKD underwent fewer cardiovascular interventions and had more in-hospital cardiovascular and bleeding events. Dual antiplatelet therapy was less likely at discharge in patients with eGFR < 30 (82.3%) than in those with ≥ 90 (91.3%) mL/min/1.73 m2 and declined more sharply during follow-up in patients with low eGFR (p < 0.0001). An adjusted proportional hazards model showed that patients with lower eGFR levels had a higher risk of cardiovascular events and bleeding.
Conclusions: The presence of CKD in patients with ACS was associated with less aggressive cardiovascular management and an increased risk of cardiovascular events.
Conflict of interest statement
F. Van de Werf has received consulting fees and research grants from Boehringer Ingelheim and Merck and consulting fees from Roche, Sanofi-Aventis, AstraZeneca, and The Medicines Company. S.J. Pocock has received research funding from AstraZeneca. C.T. Chin has received research support from Eli Lilly and honoraria from Medtronic and has been a consultant or advisory board member for AstraZeneca. A.M. Vega is a former employee of AstraZeneca. J. Medina is an employee of AstraZeneca. H. Bueno receives research funding from the Instituto de Salud Carlos III, Spain (PIE16/00021 and PI17/01799), Sociedad Española de Cardiología, AstraZeneca, Bayer, BMS, and Novartis; has received consulting fees from AstraZeneca, Bayer, BMS-Pfizer, and Novartis; and speaking fees or support for attending scientific meetings from Amgen, AstraZeneca, Bayer, BMS-Pfizer, Novartis, and MEDSCAPE-the heart.org. X. Rossello has received support from the SEC-CNIC CARDIOJOVEN fellowship program. Y. Huo, Y. Han, S. W.-L. Lee, Y. Li, and J. Jiang have no conflicts of interest that are directly relevant to the content of this article. AstraZeneca reviewed the manuscript during development and could make suggestions; however, final content, opinions, conclusions, and interpretation of the data are the responsibility of the authors. Professor Huo had full access to all of the data in the studies and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Figures
References
-
- Washam JB, Herzog CA, Beitelshees AL, Cohen MG, Henry TD, Kapur NK, et al. Pharmacotherapy in chronic kidney disease patients presenting with acute coronary syndrome: a scientific statement from the American Heart Association. Circulation. 2015;131(12):1123–1149. - PubMed
-
- Fox CS, Muntner P, Chen AY, Alexander KP, Roe MT, Cannon CP, et al. Use of evidence-based therapies in short-term outcomes of ST-segment elevation myocardial infarction and non-ST-segment elevation myocardial infarction in patients with chronic kidney disease: a report from the National Cardiovascular Data Acute Coronary Treatment and Intervention Outcomes Network registry. Circulation. 2010;121(3):357–365. - PMC - PubMed
-
- Goldenberg I, Subirana I, Boyko V, Vila J, Elosua R, Permanyer-Miralda G, et al. Relation between renal function and outcomes in patients with non-ST-segment elevation acute coronary syndrome: real-world data from the European Public Health Outcome Research and Indicators Collection Project. Arch Intern Med. 2010;170(10):888–895. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
