

Associations of Left Atrial Function and Structure With Supraventricular Ectopy: The Multi-Ethnic Study of Atherosclerosis
- PMID: 33538182
- PMCID: PMC7955336
- DOI: 10.1161/JAHA.120.018093
Associations of Left Atrial Function and Structure With Supraventricular Ectopy: The Multi-Ethnic Study of Atherosclerosis
Abstract
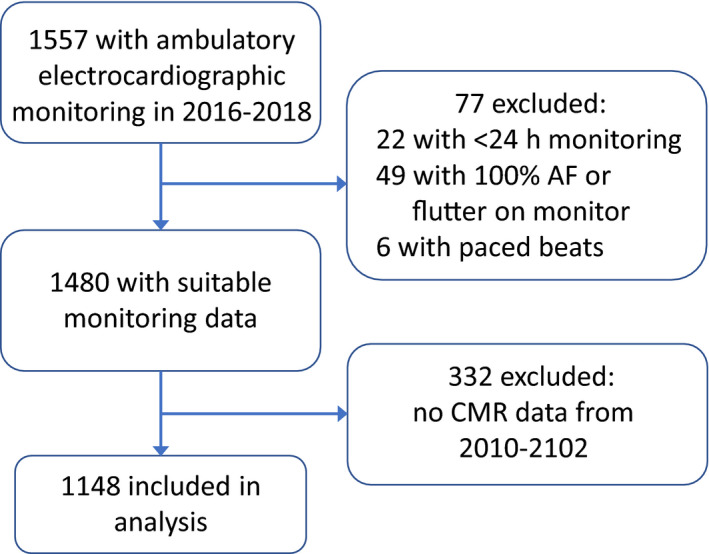
Background High levels of supraventricular ectopy are associated with greater risk of atrial fibrillation, stroke, and death. Little information is available about differences by race/ethnicity in the extent of supraventricular ectopy, or about whether high levels of supraventricular ectopy are associated with impaired left atrial (LA) function and LA enlargement. Methods and Results In the MESA (Multi-Ethnic Study of Atherosclerosis), 1148 participants (47% men; mean age, 67 years) had cardiovascular magnetic resonance imaging in 2010 to 2012, followed by 14-day ambulatory electrocardiographic monitoring in 2016 to 2018. We analyzed participant characteristics and cardiovascular magnetic resonance measures of LA function and structure in relation to average count of premature atrial contractions (PACs) per hour and average number of runs per day of supraventricular tachycardia. In adjusted regression analyses, older age, male sex, White race, elevated NT-proBNP (N-terminal pro-B-type natriuretic peptide), and a history of clinically detected atrial fibrillation were associated with more PACs/hour. Chinese and Hispanic participants had on average fewer PACs/hour than White participants (Chinese participants, 31% less [95% CI, 8%-49%]; Hispanic participants, 38% less [95% CI, 19%-52%]). Greater LA total emptying fraction was associated with fewer PACs/hour (per SD, 16% fewer PACs/hour [95% CI, 7%-25% fewer PACs/hour]). Larger LA minimum volume was associated with more PACs/hour (per SD, 7% more PACs/hour [95% CI, 2%-13% more PACs/hour]). Associations of LA volumes with runs of supraventricular tachycardia/day were similar in direction but were weaker. Conclusions Impaired LA function and LA enlargement were associated with more PACs/hour on extended ambulatory electrocardiographic monitoring. Measurement of supraventricular ectopy may provide information about the extent of atrial myopathy.
Keywords: emptying fraction; left atrium; strain; supraventricular ectopy; volume.
Conflict of interest statement
None.
Figures

References
-
- Conen D, Adam M, Roche F, Barthelemy J‐C, Felber Dietrich D, Imboden M, Künzli N, von Eckardstein A, Regenass S, Hornemann T, et al. Premature atrial contractions in the general population: frequency and risk factors. Circulation. 2012;126:2302–2308. DOI: 10.1161/CIRCULATIONAHA.112.112300. - DOI - PubMed
-
- Glotzer TV, Hellkamp AS, Zimmerman J, Sweeney MO, Yee R, Marinchak R, Cook J, Paraschos A, Love J, Radoslovich G, et al. Atrial high rate episodes detected by pacemaker diagnostics predict death and stroke: report of the Atrial Diagnostics Ancillary Study of the MOde Selection Trial (MOST). Circulation. 2003;107:1614–1619. DOI: 10.1161/01.CIR.0000057981.70380.45. - DOI - PubMed
-
- Dewland TA, Vittinghoff E, Mandyam MC, Heckbert SR, Siscovick DS, Stein PK, Psaty BM, Sotoodehnia N, Gottdiener JS, Marcus GM. Atrial ectopy as a predictor of incident atrial fibrillation: a cohort study. Ann Intern Med. 2013;159:721–728. DOI: 10.7326/0003-4819-159-11-201312030-00004. - DOI - PMC - PubMed
-
- Larsen BS, Kumarathurai P, Falkenberg J, Nielsen OW, Sajadieh A. Excessive atrial ectopy and short atrial runs increase the risk of stroke beyond incident atrial fibrillation. J Am Coll Cardiol. 2015;66:232–241. - PubMed
Publication types
MeSH terms
Grants and funding
- N01 HC095163/HC/NHLBI NIH HHS/United States
- N01 HC095168/HC/NHLBI NIH HHS/United States
- N01 HC095162/HC/NHLBI NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- N01 HC095169/HC/NHLBI NIH HHS/United States
- N01 HC095159/HC/NHLBI NIH HHS/United States
- N01 HC095161/HC/NHLBI NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- N01 HC095166/HC/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095167/HC/NHLBI NIH HHS/United States
- N01 HC095164/HC/NHLBI NIH HHS/United States
- R01 HL127659/HL/NHLBI NIH HHS/United States
- N01 HC095160/HC/NHLBI NIH HHS/United States
- R01 HL142599/HL/NHLBI NIH HHS/United States
- N01 HC095165/HC/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
