

Machine Learning-Based Early Warning Systems for Clinical Deterioration: Systematic Scoping Review
- PMID: 33538696
- PMCID: PMC7892287
- DOI: 10.2196/25187
Machine Learning-Based Early Warning Systems for Clinical Deterioration: Systematic Scoping Review
Abstract
Background: Timely identification of patients at a high risk of clinical deterioration is key to prioritizing care, allocating resources effectively, and preventing adverse outcomes. Vital signs-based, aggregate-weighted early warning systems are commonly used to predict the risk of outcomes related to cardiorespiratory instability and sepsis, which are strong predictors of poor outcomes and mortality. Machine learning models, which can incorporate trends and capture relationships among parameters that aggregate-weighted models cannot, have recently been showing promising results.
Objective: This study aimed to identify, summarize, and evaluate the available research, current state of utility, and challenges with machine learning-based early warning systems using vital signs to predict the risk of physiological deterioration in acutely ill patients, across acute and ambulatory care settings.
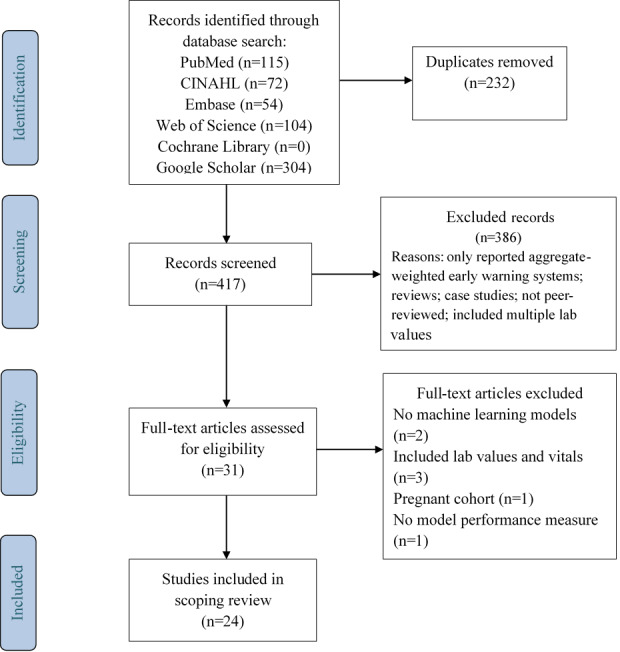
Methods: PubMed, CINAHL, Cochrane Library, Web of Science, Embase, and Google Scholar were searched for peer-reviewed, original studies with keywords related to "vital signs," "clinical deterioration," and "machine learning." Included studies used patient vital signs along with demographics and described a machine learning model for predicting an outcome in acute and ambulatory care settings. Data were extracted following PRISMA, TRIPOD, and Cochrane Collaboration guidelines.
Results: We identified 24 peer-reviewed studies from 417 articles for inclusion; 23 studies were retrospective, while 1 was prospective in nature. Care settings included general wards, intensive care units, emergency departments, step-down units, medical assessment units, postanesthetic wards, and home care. Machine learning models including logistic regression, tree-based methods, kernel-based methods, and neural networks were most commonly used to predict the risk of deterioration. The area under the curve for models ranged from 0.57 to 0.97.
Conclusions: In studies that compared performance, reported results suggest that machine learning-based early warning systems can achieve greater accuracy than aggregate-weighted early warning systems but several areas for further research were identified. While these models have the potential to provide clinical decision support, there is a need for standardized outcome measures to allow for rigorous evaluation of performance across models. Further research needs to address the interpretability of model outputs by clinicians, clinical efficacy of these systems through prospective study design, and their potential impact in different clinical settings.
Keywords: acute care; ambulatory care; cardiorespiratory instability; clinical deterioration; early warning systems; machine learning; remote patient monitoring; risk prediction; sepsis; vital signs.
©Sankavi Muralitharan, Walter Nelson, Shuang Di, Michael McGillion, PJ Devereaux, Neil Grant Barr, Jeremy Petch. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 04.02.2021.
Conflict of interest statement
Conflicts of Interest: PJD is a member of a research group with a policy of not accepting honorariums or other payments from industry for their own personal financial gain. They do accept honorariums/payments from industry to support research endeavours and costs to participate in meetings.
Based on study questions PJD has originated and grants he has written, he has received grants from Abbott Diagnostics, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers-Squibb, Coviden, Octapharma, Philips Healthcare, Roche Diagnostics, Siemens, and Stryker.
PJD has participated in advisory board meetings for GlaxoSmithKline, Boehringer Ingelheim, Bayer, and Quidel Canada. He also attended an expert panel meeting with AstraZeneca and Boehringer Ingelheim.
The other authors declare no conflicts of interest.
Figures
References
-
- Barfod C, Lauritzen MMP, Danker JK, Sölétormos G, Forberg JL, Berlac PA, Lippert F, Lundstrøm LH, Antonsen K, Lange KHW. Abnormal vital signs are strong predictors for intensive care unit admission and in-hospital mortality in adults triaged in the emergency department - a prospective cohort study. Scand J Trauma Resusc Emerg Med. 2012 Apr 10;20:28. doi: 10.1186/1757-7241-20-28. https://sjtrem.biomedcentral.com/articles/10.1186/1757-7241-20-28 - DOI - DOI - PMC - PubMed
-
- McGaughey J, Alderdice F, Fowler R, Kapila A, Mayhew A, Moutray M. Outreach and Early Warning Systems (EWS) for the prevention of intensive care admission and death of critically ill adult patients on general hospital wards. Cochrane Database Syst Rev. 2007 Jul 18;(3):CD005529. doi: 10.1002/14651858.CD005529.pub2. - DOI - PubMed
-
- Gardner-Thorpe J, Love N, Wrightson J, Walsh S, Keeling N. The value of Modified Early Warning Score (MEWS) in surgical in-patients: a prospective observational study. Ann R Coll Surg Engl. 2006 Oct;88(6):571–5. doi: 10.1308/003588406X130615. http://europepmc.org/abstract/MED/17059720 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
