

Classification and Personalized Prognostic Assessment on the Basis of Clinical and Genomic Features in Myelodysplastic Syndromes
- PMID: 33539200
- PMCID: PMC8078359
- DOI: 10.1200/JCO.20.01659
Classification and Personalized Prognostic Assessment on the Basis of Clinical and Genomic Features in Myelodysplastic Syndromes
Abstract
Purpose: Recurrently mutated genes and chromosomal abnormalities have been identified in myelodysplastic syndromes (MDS). We aim to integrate these genomic features into disease classification and prognostication.
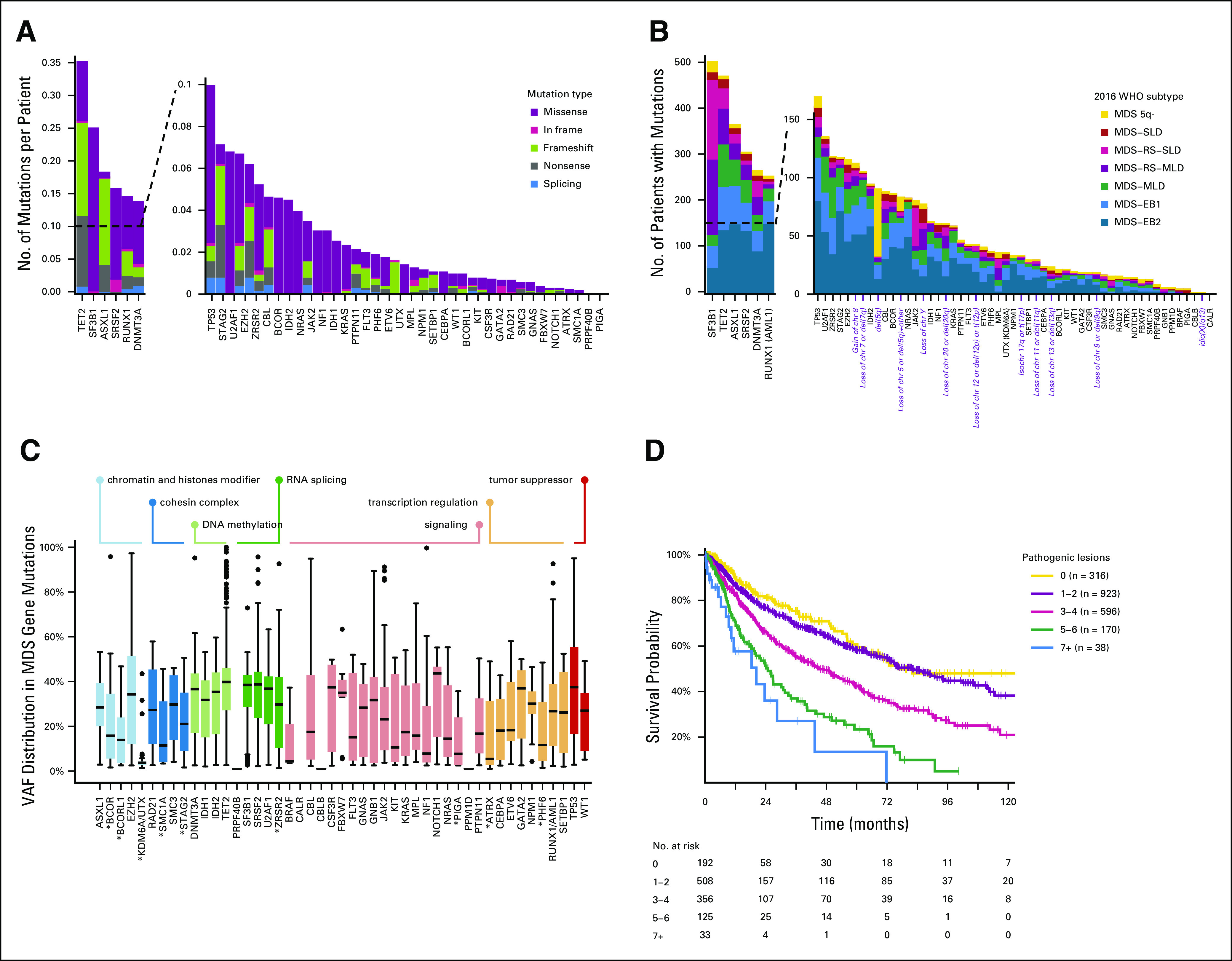
Methods: We retrospectively enrolled 2,043 patients. Using Bayesian networks and Dirichlet processes, we combined mutations in 47 genes with cytogenetic abnormalities to identify genetic associations and subgroups. Random-effects Cox proportional hazards multistate modeling was used for developing prognostic models. An independent validation on 318 cases was performed.
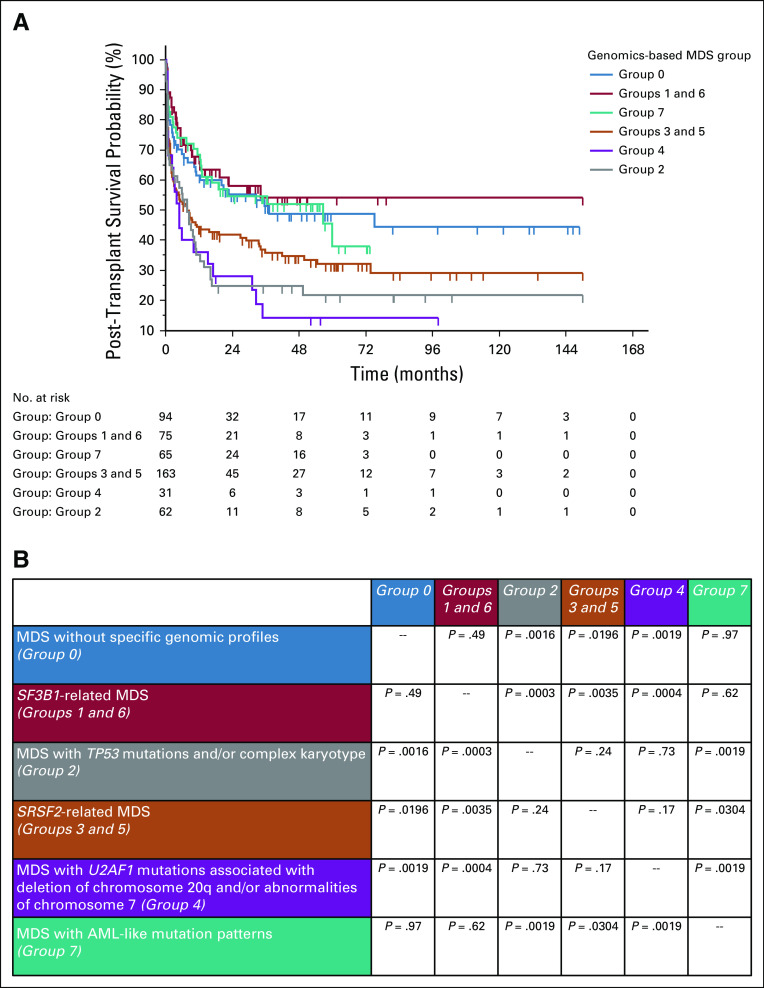
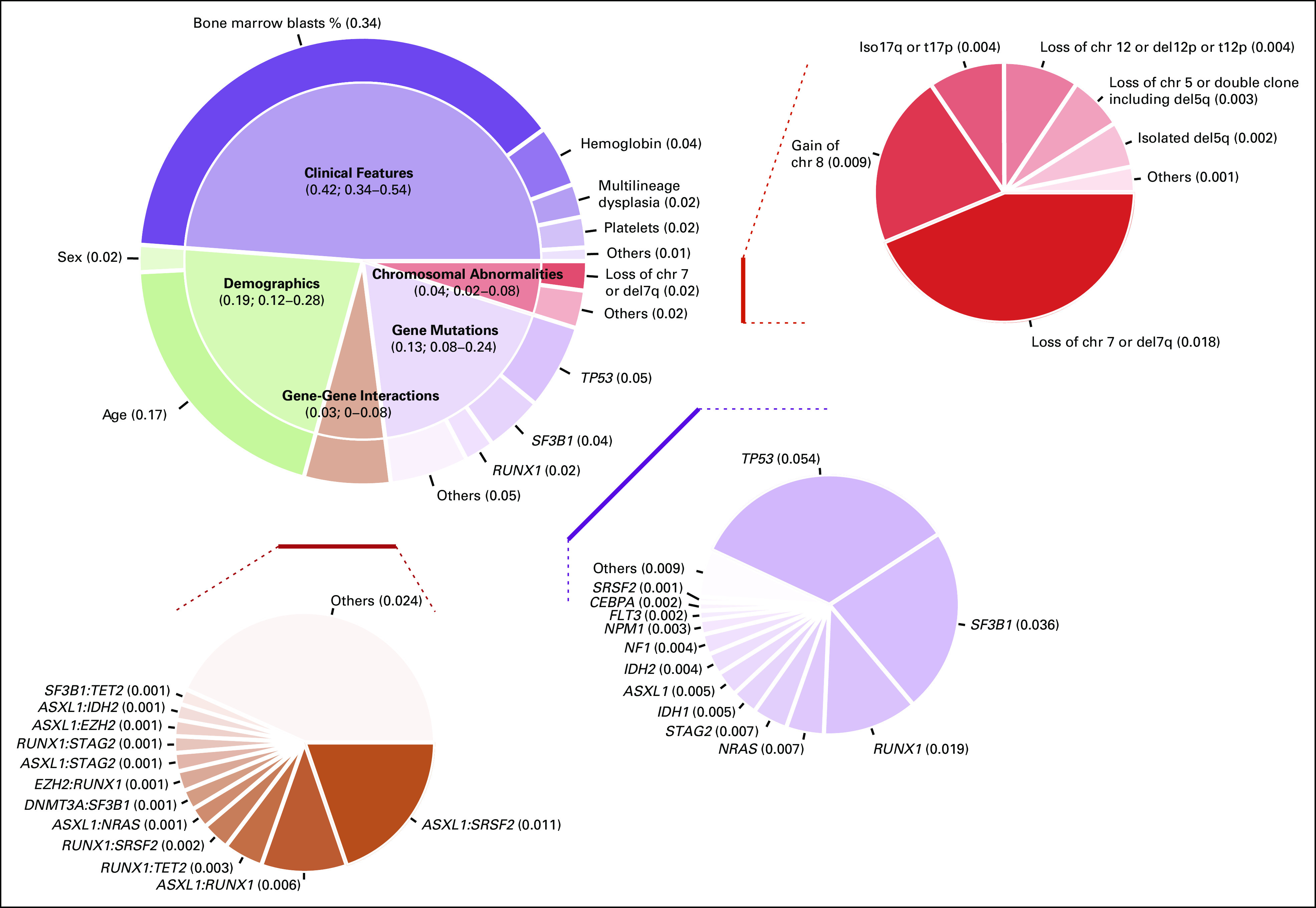
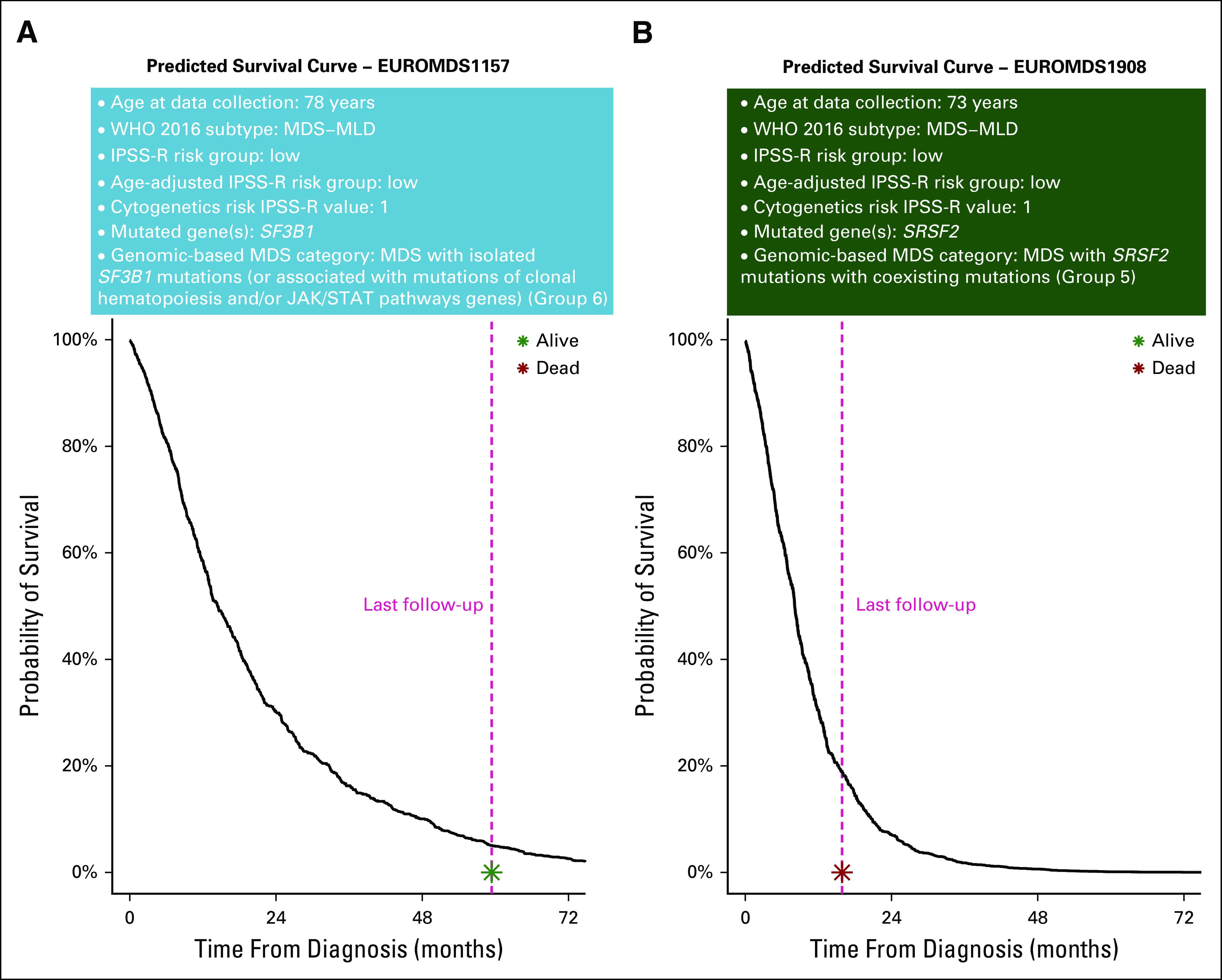
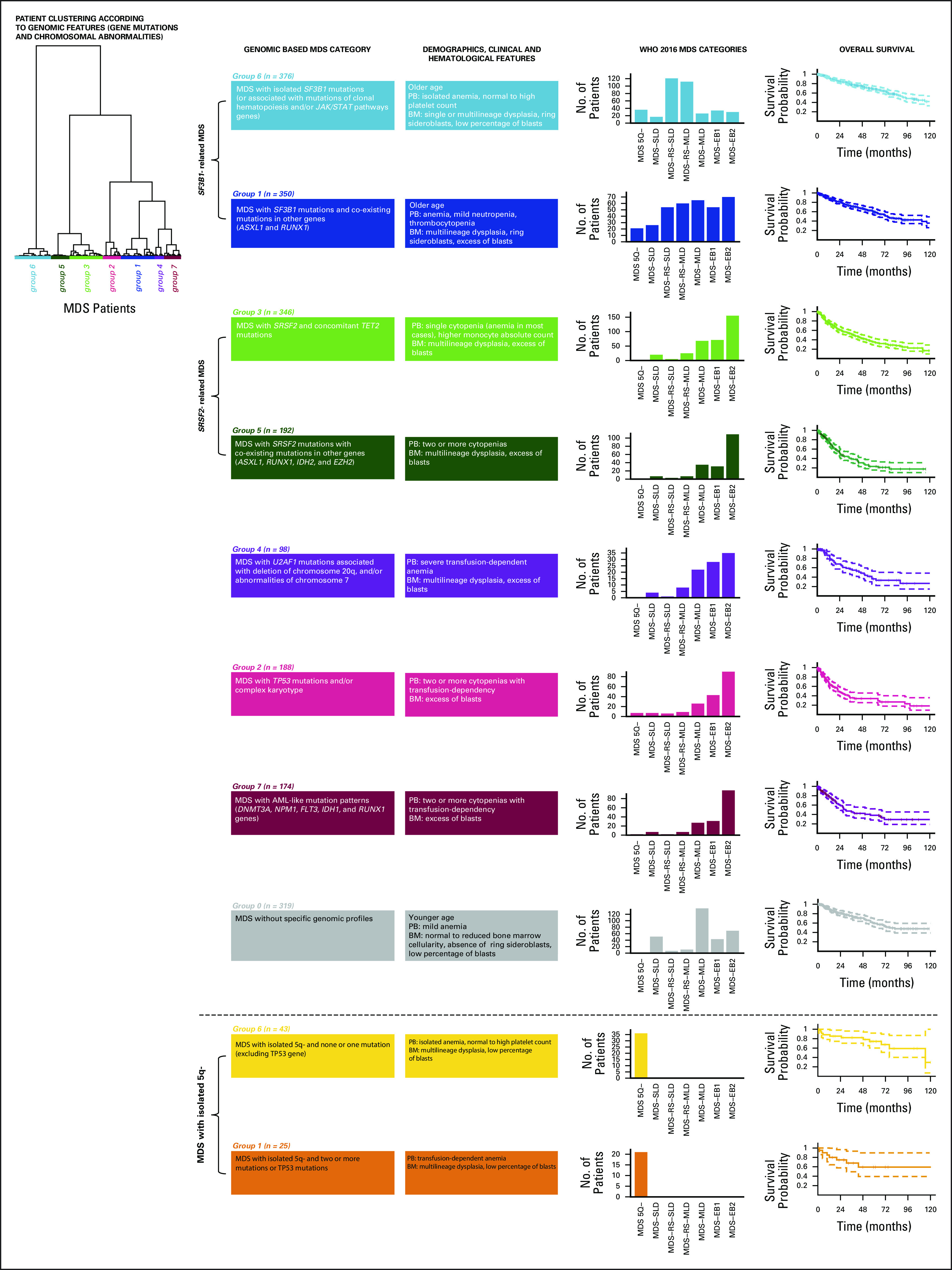
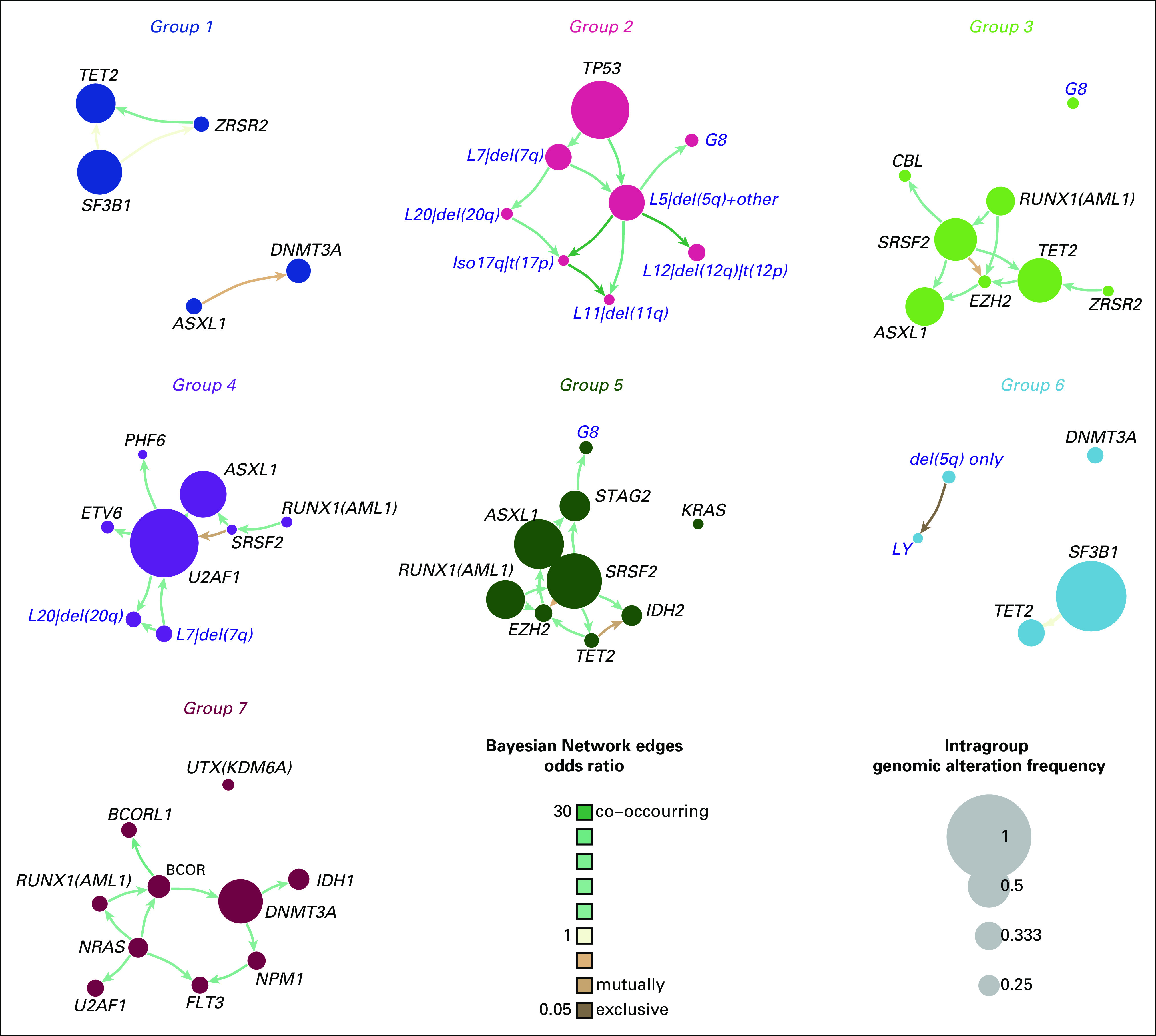
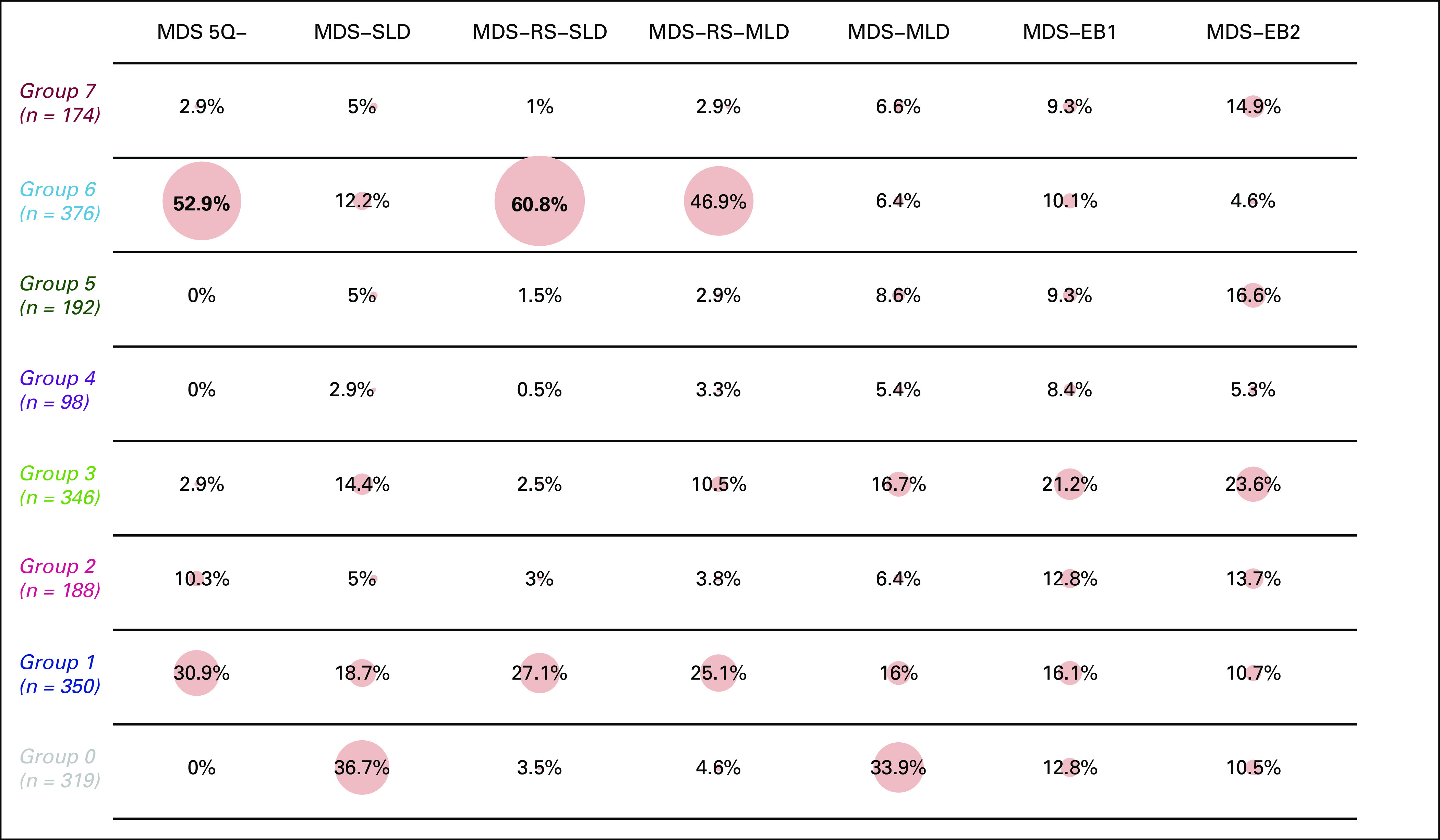
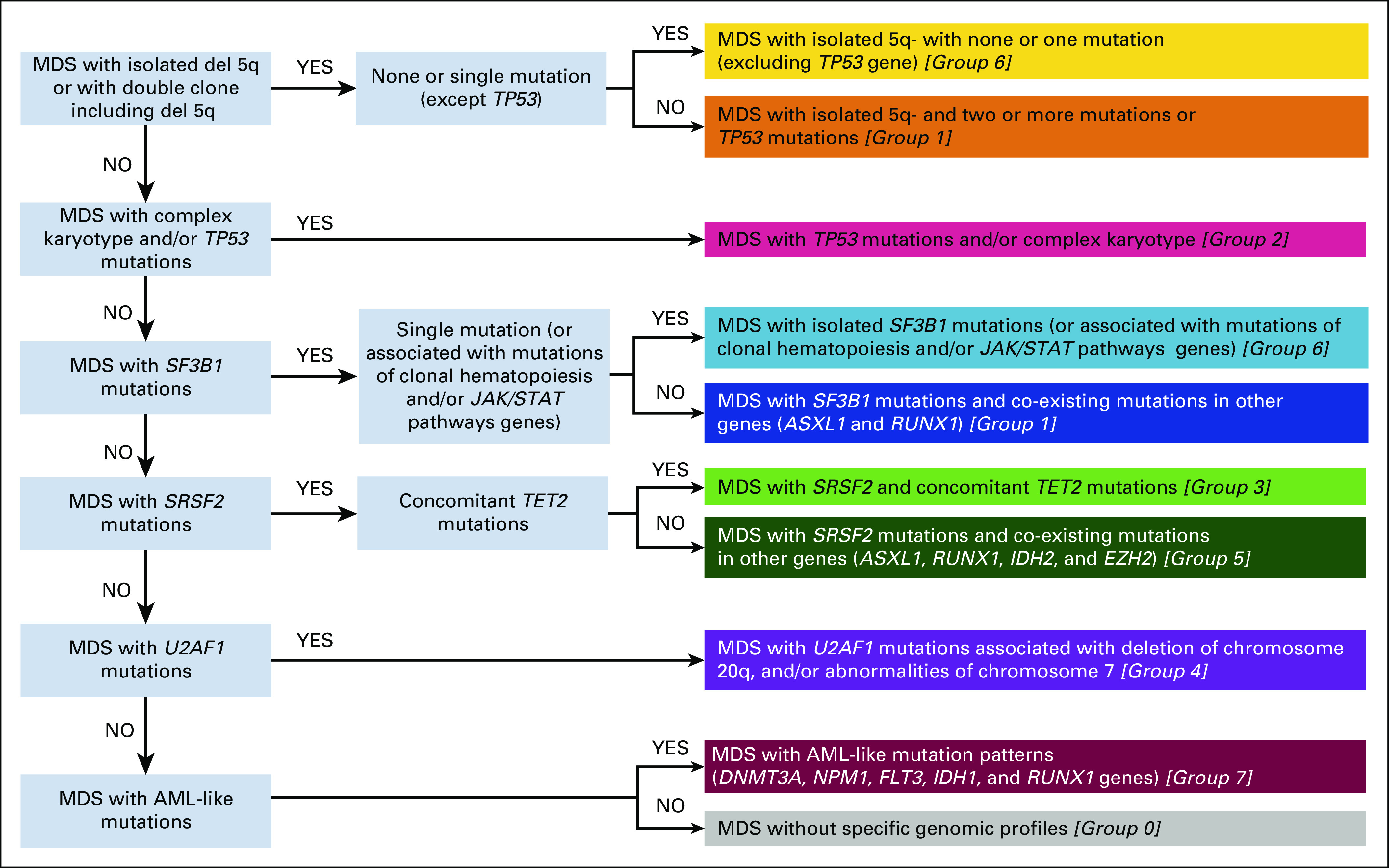
Results: We identify eight MDS groups (clusters) according to specific genomic features. In five groups, dominant genomic features include splicing gene mutations (SF3B1, SRSF2, and U2AF1) that occur early in disease history, determine specific phenotypes, and drive disease evolution. These groups display different prognosis (groups with SF3B1 mutations being associated with better survival). Specific co-mutation patterns account for clinical heterogeneity within SF3B1- and SRSF2-related MDS. MDS with complex karyotype and/or TP53 gene abnormalities and MDS with acute leukemia-like mutations show poorest prognosis. MDS with 5q deletion are clustered into two distinct groups according to the number of mutated genes and/or presence of TP53 mutations. By integrating 63 clinical and genomic variables, we define a novel prognostic model that generates personally tailored predictions of survival. The predicted and observed outcomes correlate well in internal cross-validation and in an independent external cohort. This model substantially improves predictive accuracy of currently available prognostic tools. We have created a Web portal that allows outcome predictions to be generated for user-defined constellations of genomic and clinical features.
Conclusion: Genomic landscape in MDS reveals distinct subgroups associated with specific clinical features and discrete patterns of evolution, providing a proof of concept for next-generation disease classification and prognosis.
Conflict of interest statement
Figures
References
-
- Adès L, Itzykson R, Fenaux P: Myelodysplastic syndromes. Lancet 383:2239-2252, 2014 - PubMed
-
- Arber DA Orazi A Hasserjian R, et al. : The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 127:2391-2405, 2016 - PubMed
-
- Della Porta MG Travaglino E Boveri E, et al. : Minimal morphological criteria for defining bone marrow dysplasia: A basis for clinical implementation of WHO classification of myelodysplastic syndromes. Leukemia 29:66-75, 2015 - PubMed
-
- Malcovati L Della Porta MG Pascutto C, et al. : Prognostic factors and life expectancy in myelodysplastic syndromes classified according to WHO criteria: A basis for clinical decision making. J Clin Oncol 23:7594-7603, 2005 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
