

Myocardial deformation assessed among heart failure entities by cardiovascular magnetic resonance imaging
- PMID: 33539681
- PMCID: PMC8006725
- DOI: 10.1002/ehf2.13193
Myocardial deformation assessed among heart failure entities by cardiovascular magnetic resonance imaging
Abstract
Aims: Although heart failure (HF) is a leading cause for hospitalization and mortality, normalized and comparable non-invasive assessment of haemodynamics and myocardial action remains limited. Moreover, myocardial deformation has not been compared between the guideline-defined HF entities. The distribution of affected and impaired segments within the contracting left ventricular (LV) myocardium have also not been compared. Therefore, we assessed myocardial function impairment by strain in patients with HF and control subjects by magnetic resonance imaging after clinically phenotyping these patients.
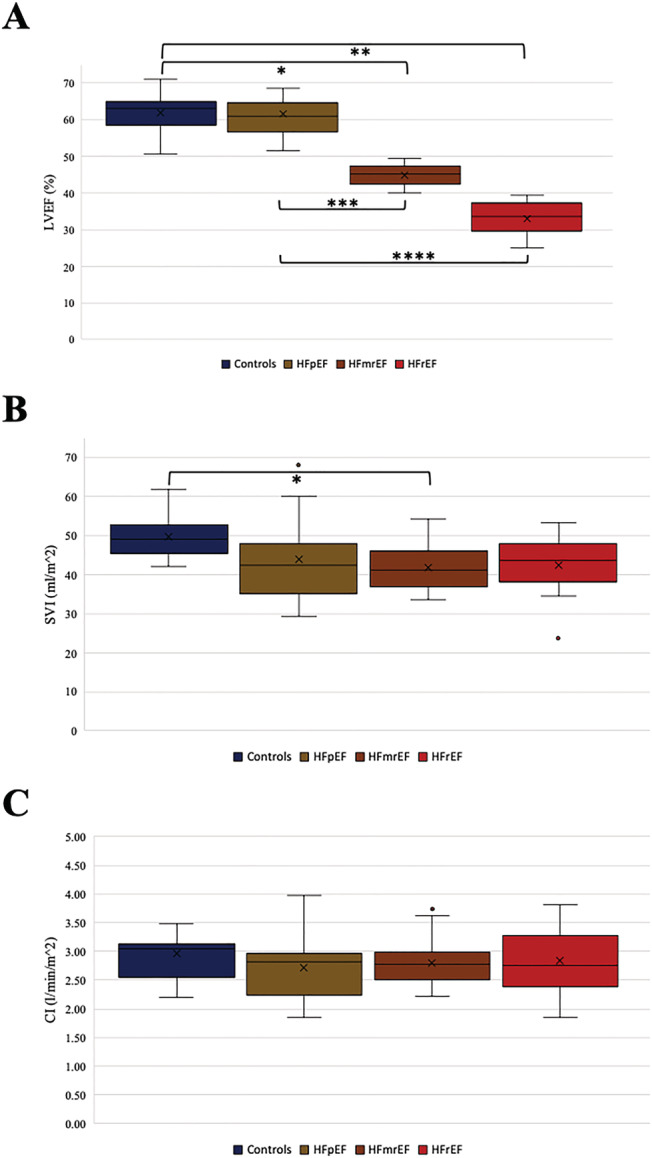
Methods and results: This prospective study conducted at two centres in Germany between 2017 and 2018 enrolled stable outpatient subjects with HF [n = 56, including HF with reduced ejection fraction (HFrEF), HF with mid-range ejection fraction (HFmrEF), and HF with preserved ejection fraction (HFpEF)] and a control cohort (n = 12). Parameters assessed included measures for external myocardial function, for example, cardiac index and myocardial deformation measurements by cardiovascular magnetic resonance imaging, left ventricular global longitudinal strain (GLS), the global circumferential strain (GCS) and the regional distribution of segment deformation within the LV myocardium, as well as basic phenotypical characteristics. Comparison of the cardiac indices at rest showed no differences neither between the HF groups nor between the control group and HF patients (one-way ANOVA P = 0.70). The analysis of the strain data revealed differences between all groups in both LV GLS (One-way ANOVA: P < 0.01. Controls vs. HFpEF: -20.48 ± 1.62 vs. -19.27 ± 1.25. HFpEF vs. HFmrEF: -19.27 ± 1.25 vs. -15.72 ± 2.76. HFmrEF vs. HFrEF: -15.72 ± 2.76 vs. -11.51 ± 3.97.) and LV GCS (One-way ANOVA: P < 0.01. Controls vs. HFpEF: -19.74 ± 2.18 vs. -17.47 ± 2.10. HFpEF vs. HFmrEF: -17.47 ± 2.10 vs. -12.78 ± 3.47. HFrEF: -11.41 ± 3.27). Comparing the segment deformation distribution patterns highlighted the discriminating effect between the groups was much more prominent between the groups (one-way ANOVA P < 0.01) when compared by a score combining regional effects and a global view on the LV. Further analyses of the patterns among the segments affected showed that while the LVEF is preserved in HFpEF, the segments impaired in their contractility are located in the ventricular septum. The worse the LVEF is, the more segments are affected, but the septum remains an outstanding location with the most severe contractility impairment throughout the HF entities.
Conclusions: While cardiac index at rest did not differ significantly between controls and stable HF patients suffering from HFrEF, HFmrEF, or HFpEF, the groups did differ significantly in LV GLS and LV GCS values. Regional strain analysis revealed that the LV septum is the location affected most, with reduced values already visible in HFpEF and further reductions in HFmrEF and HFrEF.
Keywords: CMR; Cardiac MRI; Heart failure; Myocardial deformation; Strain.
© 2021 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
S. K. reports grants and other support by the DZHK (German Center for Cardiovascular Research), Partner Site Berlin, Philips Healthcare, BioVentrix, Berlin‐Chemie, Merck/Bayer, Novartis, Astra Zeneca, Siemens, and Myocardial Solutions outside of the submitted work. S. K. is also on the advisory board for Merck/Bayer, BioVentrix, and Myocardial Solutions. B. P. has provided steering committee and advisory board services for Bayer Healthcare and MSD and has received steering committee and advisory board/speaker honoraria from Novartis. P. D. is a shareholder of Siemens and Bayer. All other authors declare that they have no relationships relevant to the contents of this paper to disclose.
Figures



References
-
- Taylor AL, Ziesche S, Yancy C, Carson P, D'Agostino R, Ferdinand K, Taylor M, Adams K, Sabolinski M, Worcel M, Cohn JN, African‐American Heart Failure Trial Investigators . Combination of isosorbide dinitrate and hydralazine in blacks with heart failure. N Engl J Med 2004; 351: 2049–2057. - PubMed
-
- Bleumink GS, Knetsch AM, Sturkenboom MCJM, Straus SMJM, Hofman A, Deckers JW, Witteman JCM, Stricker BHC. Quantifying the heart failure epidemic: prevalence, incidence rate, lifetime risk and prognosis of heart failure—the Rotterdam Study. Eur Heart J 2004; 25: 1614–1619. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González‐Juanatey JR, Harjola V‐P, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P, Authors/Task Force Members, Document Reviewers . ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution. Eur J Heart Fail 2016; 18: 891–975. - PubMed
-
- Koh AS, Tay WT, Teng THK, Vedin O, Benson L, Dahlstrom U, Savarese G, Lam CSP, Lund LH. A comprehensive population‐based characterization of heart failure with mid‐range ejection fraction. Eur J Heart Fail 2017; 19: 1624–1634. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
