

Hypofractionated radiotherapy in locally advanced bladder cancer: an individual patient data meta-analysis of the BC2001 and BCON trials
- PMID: 33539743
- PMCID: PMC7851111
- DOI: 10.1016/S1470-2045(20)30607-0
Hypofractionated radiotherapy in locally advanced bladder cancer: an individual patient data meta-analysis of the BC2001 and BCON trials
Abstract
Background: Two radiotherapy fractionation schedules are used to treat locally advanced bladder cancer: 64 Gy in 32 fractions over 6·5 weeks and a hypofractionated schedule of 55 Gy in 20 fractions over 4 weeks. Long-term outcomes of these schedules in several cohort studies and case series suggest that response, survival, and toxicity are similar, but no direct comparison has been published. The present study aimed to assess the non-inferiority of 55 Gy in 20 fractions to 64 Gy in 32 fractions in terms of invasive locoregional control and late toxicity in patients with locally advanced bladder cancer.
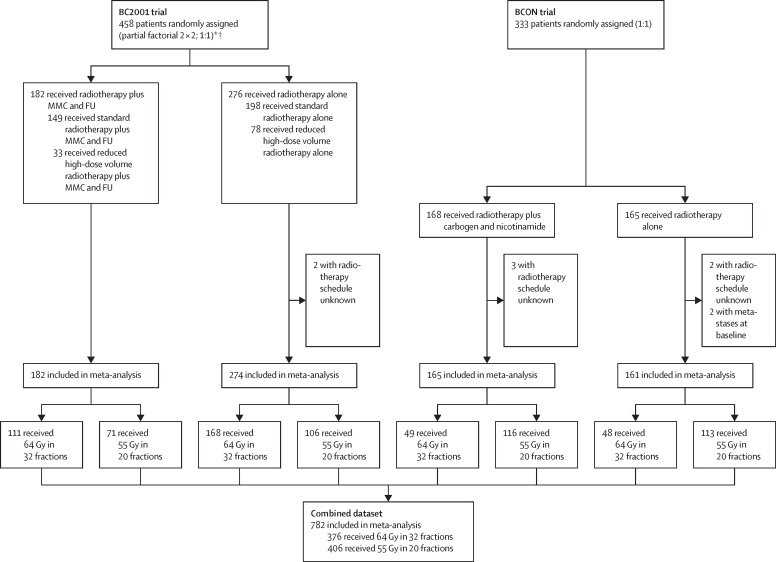
Methods: We did a meta-analysis of individual patient data from patients (age ≥18 years) with locally advanced bladder cancer (T1G3 [high-grade non-muscle invasive] or T2-T4, N0M0) enrolled in two multicentre, randomised, controlled, phase 3 trials done in the UK: BC2001 (NCT00024349; assessing addition of chemotherapy to radiotherapy) and BCON (NCT00033436; assessing hypoxia-modifying therapy combined with radiotherapy). In each trial, the fractionation schedule was chosen according to local standard practice. Co-primary endpoints were invasive locoregional control (non-inferiority margin hazard ratio [HR]=1·25); and late bladder or rectum toxicity, assessed with the Late Effects Normal Tissue Task Force-Subjective, Objective, Management, Analytic tool (non-inferiority margin for absolute risk difference [RD]=10%). If non-inferiority was met for invasive locoregional control, superiority could be considered if the 95% CI for the treatment effect excluded the null effect (HR=1). One-stage individual patient data meta-analysis models for the time-to-event and binary outcomes were used, accounting for trial differences, within-centre correlation, randomised treatment received, baseline variable imbalances, and potential confounding from relevant prognostic factors.
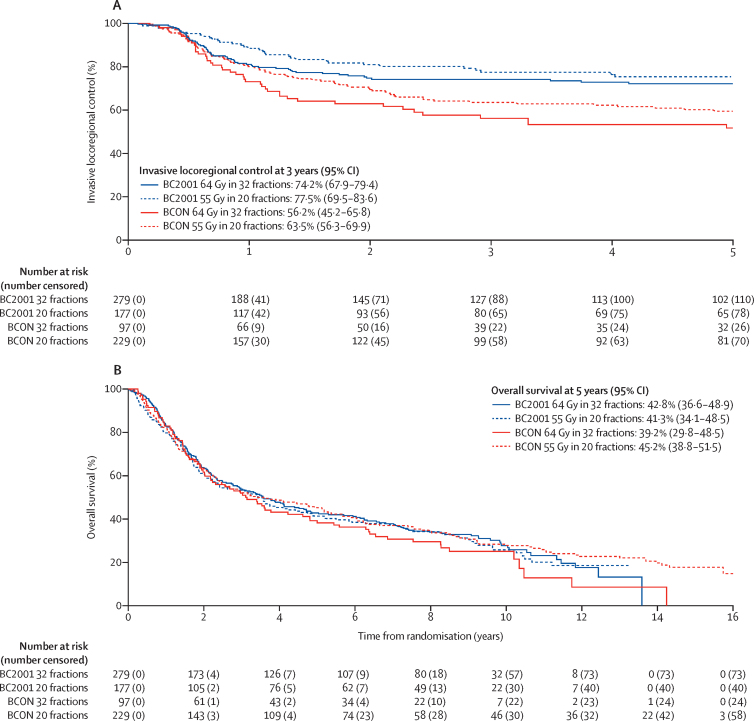
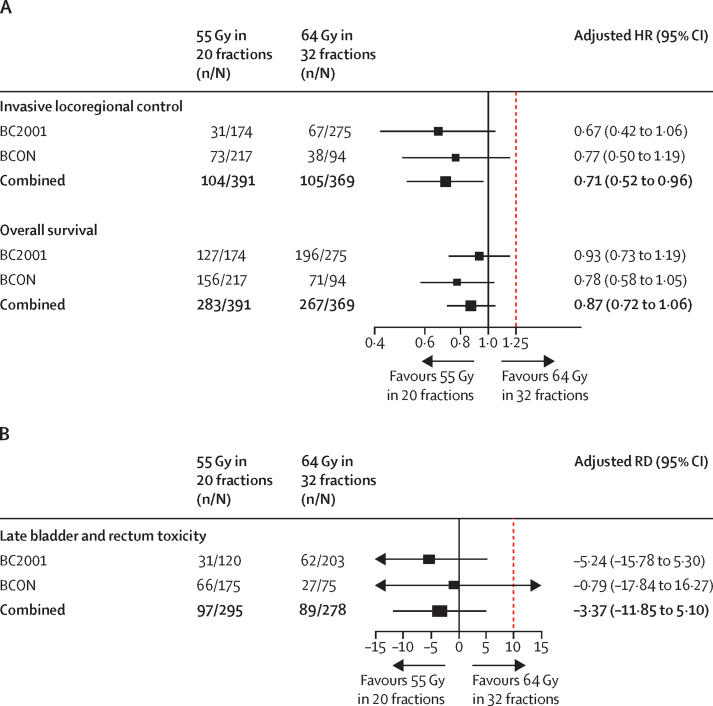
Findings: 782 patients with known fractionation schedules (456 from the BC2001 trial and 326 from the BCON trial; 376 (48%) received 64 Gy in 32 fractions and 406 (52%) received 55 Gy in 20 fractions) were included in our meta-analysis. Median follow-up was 120 months (IQR 99-159). Patients who received 55 Gy in 20 fractions had a lower risk of invasive locoregional recurrence than those who received 64 Gy in 32 fractions (adjusted HR 0·71 [95% CI 0·52-0·96]). Both schedules had similar toxicity profiles (adjusted RD -3·37% [95% CI -11·85 to 5·10]).
Interpretation: A hypofractionated schedule of 55 Gy in 20 fractions is non-inferior to 64 Gy in 32 fractions with regard to both invasive locoregional control and toxicity, and is superior with regard to invasive locoregional control. 55 Gy in 20 fractions should be adopted as a standard of care for bladder preservation in patients with locally advanced bladder cancer.
Funding: Cancer Research UK.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
[Moderate hypofractionated radiotherapy for bladder cancer-a new standard of care?].Strahlenther Onkol. 2021 Sep;197(9):854-856. doi: 10.1007/s00066-021-01804-2. Epub 2021 Jul 6. Strahlenther Onkol. 2021. PMID: 34228169 Free PMC article. German. No abstract available.
-
Standard Versus Hypofractionated Radiation Therapy for Bladder Cancer: New Insights, but Questions Remain.Int J Radiat Oncol Biol Phys. 2021 Sep 1;111(1):113-116. doi: 10.1016/j.ijrobp.2021.04.048. Int J Radiat Oncol Biol Phys. 2021. PMID: 34348106 Free PMC article. No abstract available.
-
Optimizing Organ Preservation Strategies in Localized Muscle Invasive Bladder Cancer.Int J Radiat Oncol Biol Phys. 2021 Dec 1;111(5):1097-1100. doi: 10.1016/j.ijrobp.2021.09.021. Int J Radiat Oncol Biol Phys. 2021. PMID: 34793725 No abstract available.
References
-
- Hoskin PJ, Rojas AM, Bentzen SM, Saunders MI. Radiotherapy with concurrent carbogen and nicotinamide in bladder carcinoma. J Clin Oncol. 2010;28:4912–4918. - PubMed
-
- Choudhury A, Swindell R, Logue JP. Phase II study of conformal hypofractionated radiotherapy with concurrent gemcitabine in muscle-invasive bladder cancer. J Clin Oncol. 2011;29:733–738. - PubMed
-
- James ND, Hussain SA, Hall E. Radiotherapy with or without chemotherapy in muscle-invasive bladder cancer. N Engl J Med. 2012;366:1477–1488. - PubMed
-
- Booth CM, Siemens DR, Li G. Curative therapy for bladder cancer in routine clinical practice: a population-based outcomes study. Clin Oncol (R Coll Radiol) 2014;26:506–514. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
