

Dose of Continuous Renal Replacement Therapy in Critically Ill Patients: A Bona Fide Quality Indicator
- PMID: 33540417
- PMCID: PMC7965247
- DOI: 10.1159/000512846
Dose of Continuous Renal Replacement Therapy in Critically Ill Patients: A Bona Fide Quality Indicator
Abstract
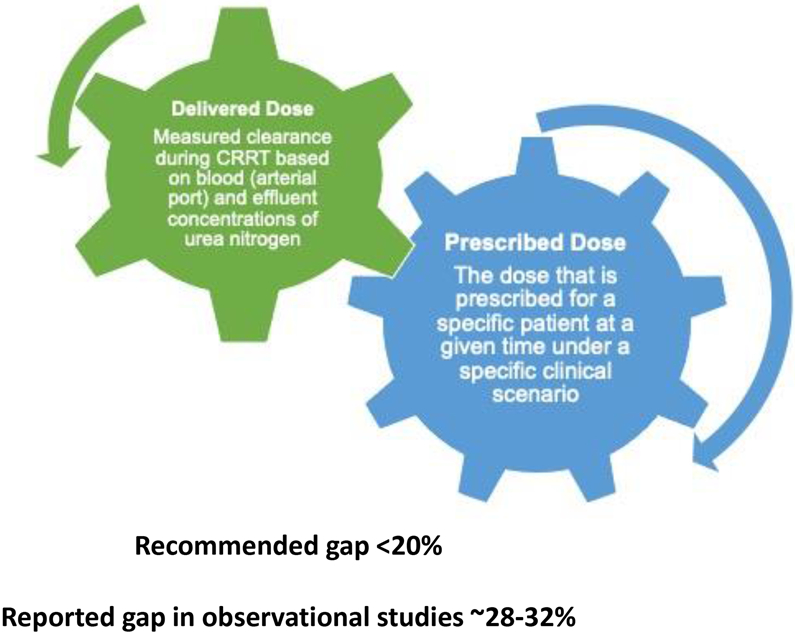
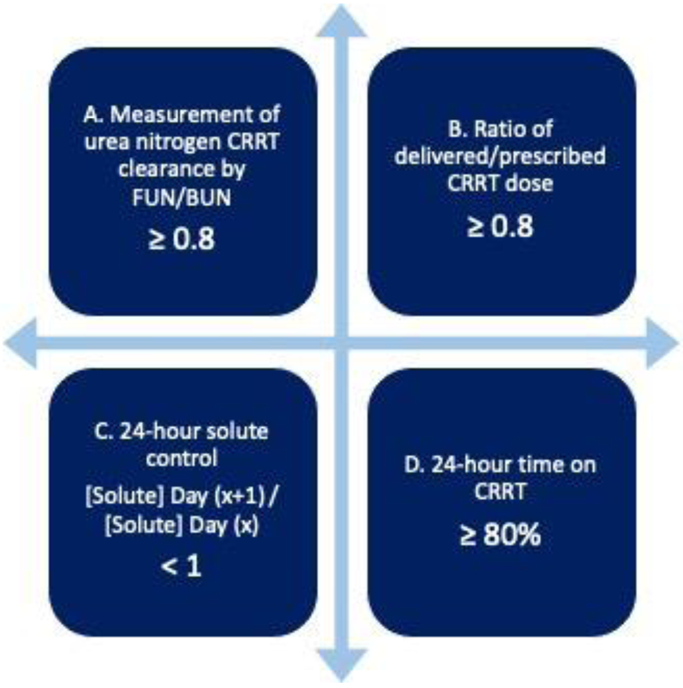
Acute kidney injury (AKI) is common in critically ill patients, and renal replacement therapy (RRT) constitutes an important aspect of acute management during critical illness. Continuous RRT (CRRT) is frequently utilized in intensive care unit settings, particularly in patients with severe AKI, fluid overload, and hemodynamic instability. The main goal of CRRT is to timely optimize solute control, acid-base, and volume status. Total effluent dose of CRRT is a deliverable that depends on multiple factors and therefore should be systematically monitored (prescribed vs. delivered) and iteratively adjusted in a sustainable mode. In this manuscript, we review current evidence of CRRT dosing and provide recommendations for its implementation as a quality indicator of CRRT delivery.
Keywords: Acute kidney injury; Continuous renal replacement therapy; Dose; Quality indicator; Quality metric.
© 2021 S. Karger AG, Basel.
Conflict of interest statement
Conflict of Interest
Dr. Neyra has consulted for Baxter Healthcare and Renibus Therapeutics.
Figures
Similar articles
-
Delivered dose of renal replacement therapy and mortality in critically ill patients with acute kidney injury.Crit Care. 2009;13(2):R57. doi: 10.1186/cc7784. Epub 2009 Apr 15. Crit Care. 2009. PMID: 19368724 Free PMC article.
-
Initial renal replacement therapy (RRT) modality associates with 90-day postdischarge RRT dependence in critically ill AKI survivors.J Crit Care. 2024 Aug;82:154764. doi: 10.1016/j.jcrc.2024.154764. Epub 2024 Mar 8. J Crit Care. 2024. PMID: 38460295
-
Renal replacement therapy for AKI: When? How much? When to stop?Best Pract Res Clin Anaesthesiol. 2017 Sep;31(3):371-385. doi: 10.1016/j.bpa.2017.10.001. Epub 2017 Nov 1. Best Pract Res Clin Anaesthesiol. 2017. PMID: 29248144 Review.
-
CRRT prescription and delivery of dose.Semin Dial. 2021 Nov;34(6):432-439. doi: 10.1111/sdi.12974. Epub 2021 Apr 28. Semin Dial. 2021. PMID: 33909931
-
Intensity of renal replacement therapy and outcomes in critically ill patients with acute kidney injury: Critical appraisal of the dosing recommendations.Ther Apher Dial. 2020 Dec;24(6):620-627. doi: 10.1111/1744-9987.13471. Epub 2020 Feb 8. Ther Apher Dial. 2020. PMID: 31904909 Review.
Cited by
-
Lacosamide dosing in patients receiving continuous renal replacement therapy.J Intensive Care. 2023 Nov 9;11(1):50. doi: 10.1186/s40560-023-00700-4. J Intensive Care. 2023. PMID: 37946296 Free PMC article.
-
Can Artificial Intelligence Assist in Delivering Continuous Renal Replacement Therapy?Adv Chronic Kidney Dis. 2022 Sep;29(5):439-449. doi: 10.1053/j.ackd.2022.08.001. Adv Chronic Kidney Dis. 2022. PMID: 36253027 Free PMC article. Review.
-
CKRT coagulation risk prediction and nursing feedback model based on intelligent algorithms.BMC Nephrol. 2025 Jul 24;26(1):414. doi: 10.1186/s12882-025-04206-z. BMC Nephrol. 2025. PMID: 40707887 Free PMC article.
-
Lessons Learned from a Small Pediatric Continuous Renal Replacement Therapy Program.Crit Care Res Pract. 2021 Nov 17;2021:6481559. doi: 10.1155/2021/6481559. eCollection 2021. Crit Care Res Pract. 2021. PMID: 34840825 Free PMC article.
-
Continuous Renal Replacement Therapy: Application of Kidney Disease Improving Global Outcomes Guidelines for Treatment Prescription in Dogs With Acute Kidney Injury and Outcome Prediction.J Vet Intern Med. 2025 Jul-Aug;39(4):e70183. doi: 10.1111/jvim.70183. J Vet Intern Med. 2025. PMID: 40613773 Free PMC article.
References
-
- Tolwani A. Continuous renal-replacement therapy for acute kidney injury. N Engl J Med. 2012;367(26):2505–2514. - PubMed
-
- Bellomo R, Cass A, Cole L, Finfer S, Gallagher M, Lo S, McArthur C, McGuinness S, Myburgh J, Norton R, Scheinkestel C, Su S. Intensity of continuous renal-replacement therapy in critically ill patients. N Engl J Med 2009; 361: 1627–1638. - PubMed
-
- Liu KD, Himmelfarb J, Paganini E, Ikizler TA, Soroko SH, Mehta RL, Chertow GM. Timing of initiation of dialysis in critically ill patients with acute kidney injury. Clin J Am Soc Nephrol. 2006;1(5):915–919. - PubMed
-
- Saudan P, Niederberger M, De Seigneux S, Romand J, Pugin J, Perneger T, Martin PY. Adding a dialysis dose to continuous hemofiltration increases survival in patients with acute renal failure. Kidney Int. 2006;70(7):1312–1317. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
