

Prospective validation of Canadian TIA Score and comparison with ABCD2 and ABCD2i for subsequent stroke risk after transient ischaemic attack: multicentre prospective cohort study
- PMID: 33541890
- PMCID: PMC7859838
- DOI: 10.1136/bmj.n49
Prospective validation of Canadian TIA Score and comparison with ABCD2 and ABCD2i for subsequent stroke risk after transient ischaemic attack: multicentre prospective cohort study
Erratum in
-
Prospective validation of Canadian TIA Score and comparison with ABCD2 and ABCD2i for subsequent stroke risk after transient ischaemic attack: multicentre prospective cohort study.BMJ. 2021 Feb 18;372:n453. doi: 10.1136/bmj.n453. BMJ. 2021. PMID: 33602669 Free PMC article. No abstract available.
Abstract
Objective: To validate the previously derived Canadian TIA Score to stratify subsequent stroke risk in a new cohort of emergency department patients with transient ischaemic attack.
Design: Prospective cohort study.
Setting: 13 Canadian emergency departments over five years.
Participants: 7607 consecutively enrolled adult patients attending the emergency department with transient ischaemic attack or minor stroke.
Main outcome measures: The primary outcome was subsequent stroke or carotid endarterectomy/carotid artery stenting within seven days. The secondary outcome was subsequent stroke within seven days (with or without carotid endarterectomy/carotid artery stenting). Telephone follow-up used the validated Questionnaire for Verifying Stroke Free Status at seven and 90 days. All outcomes were adjudicated by panels of three stroke experts, blinded to the index emergency department visit.
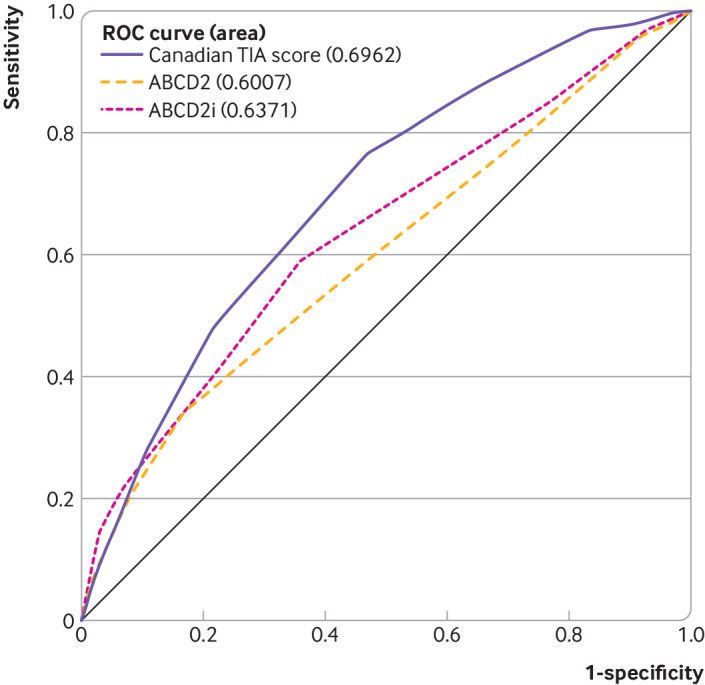
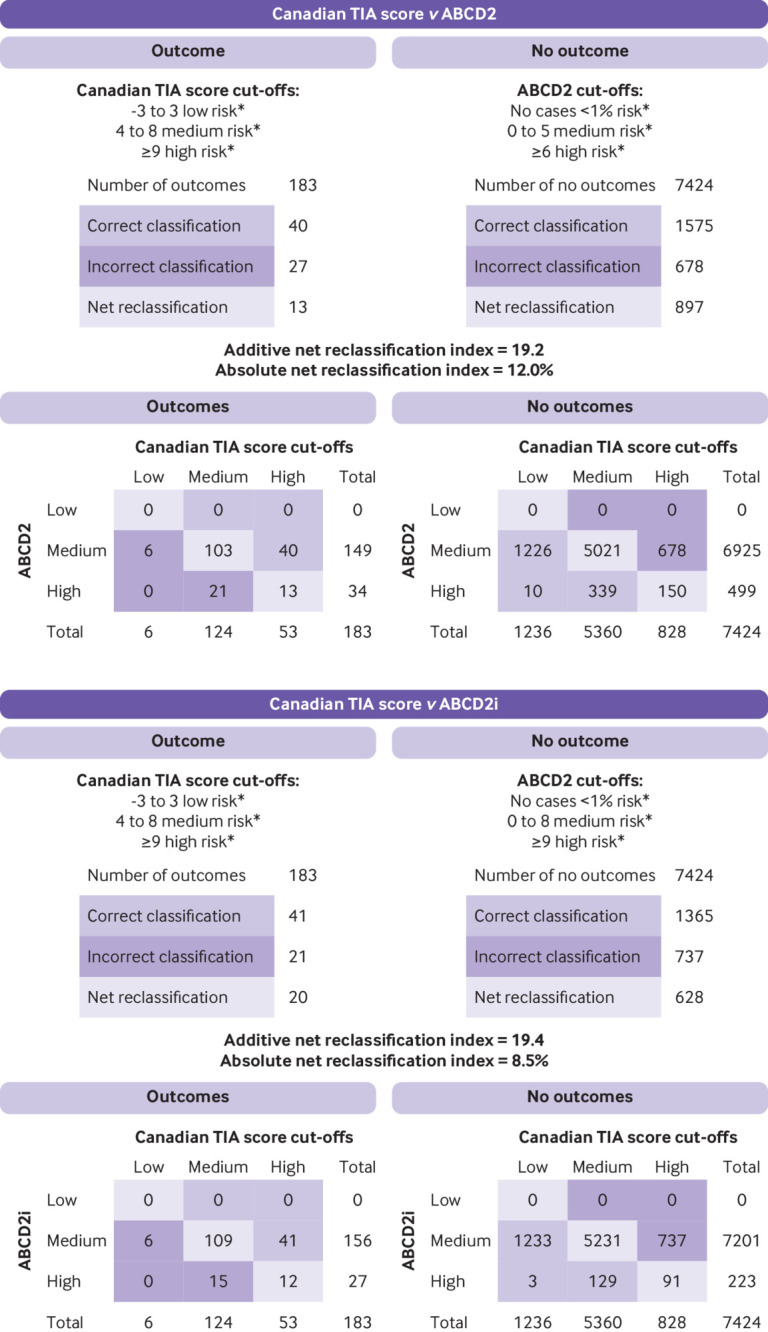
Results: Of the 7607 patients, 108 (1.4%) had a subsequent stroke within seven days, 83 (1.1%) had carotid endarterectomy/carotid artery stenting within seven days, and nine had both. The Canadian TIA Score stratified the risk of stroke, carotid endarterectomy/carotid artery stenting, or both within seven days as low (risk ≤0.5%; interval likelihood ratio 0.20, 95% confidence interval 0.09 to 0.44), medium (risk 2.3%; interval likelihood ratio 0.94, 0.85 to 1.04), and high (risk 5.9% interval likelihood ratio 2.56, 2.02 to 3.25) more accurately (area under the curve 0.70, 95% confidence interval 0.66 to 0.73) than did the ABCD2 (0.60, 0.55 to 0.64) or ABCD2i (0.64, 0.59 to 0.68). Results were similar for subsequent stroke regardless of carotid endarterectomy/carotid artery stenting within seven days.
Conclusion: The Canadian TIA Score stratifies patients' seven day risk for stroke, with or without carotid endarterectomy/carotid artery stenting, and is now ready for clinical use. Incorporating this validated risk estimate into management plans should improve early decision making at the index emergency visit regarding benefits of hospital admission, timing of investigations, and prioritisation of specialist referral.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: the study was funded by the Canadian Institutes of Health Research; JJP is supported by a mid-career award from the Heart and Stroke Foundation of Ontario; JL is supported by the Schwartz/Reisman Emergency Medicine Institute inaugural research chair in geriatric emergency medicine; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Does the Canadian TIA Score adequately risk stratify patients for subsequent stroke and revascularization in the emergency department?CJEM. 2022 Mar;24(2):131-132. doi: 10.1007/s43678-021-00221-9. Epub 2021 Nov 3. CJEM. 2022. PMID: 34734377 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical