

Cardiac arrest in a patient with trichorhinophalangeal syndrome and dilated cardiomyopathy
- PMID: 33542011
- PMCID: PMC7868179
- DOI: 10.1136/bcr-2020-237604
Cardiac arrest in a patient with trichorhinophalangeal syndrome and dilated cardiomyopathy
Abstract
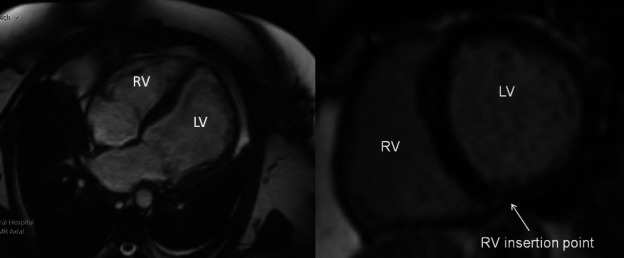
A 44-year-old woman with known trichorhinophalangeal syndrome presented with an unheralded out of hospital cardiac arrest. Transthoracic echocardiography showed severe left ventricular systolic dysfunction with an ejection fraction <25% and cardiac MRI confirmed a diagnosis of congenital non-ischaemic dilated cardiomyopathy. The case highlights a very rare syndrome, it is previously unknown association with dilated cardiomyopathy and the possible benefit of cardiac screening for patients with known trichorhinophalangeal syndrome.
Keywords: arrhythmias; cardiovascular medicine; genetic screening / counselling; heart failure; resuscitation.
© BMJ Publishing Group Limited 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
A novel base pair deletion in the TRPS1 gene in a Japanese patient with trichorhinophalangeal syndrome.Eur J Dermatol. 2018 Feb 1;28(1):107-108. doi: 10.1684/ejd.2018.3253. Eur J Dermatol. 2018. PMID: 29521629 No abstract available.
-
Incidental finding of an Xq microdeletion in a girl with trichorhinophalangeal syndrome type I harboring a novel TRPS1 nonsense mutation.Minerva Pediatr. 2018 Dec;70(6):639-642. doi: 10.23736/S0026-4946.18.05011-9. Epub 2018 Apr 12. Minerva Pediatr. 2018. PMID: 29651829 No abstract available.
-
Thricho-rhino-phalangeal syndrome and severe osteoporosis: a rare association or a feature? An effective therapeutic approach with biphosphonates.Am J Med Genet A. 2014 Mar;164A(3):760-3. doi: 10.1002/ajmg.a.36327. Epub 2013 Dec 19. Am J Med Genet A. 2014. PMID: 24357341
-
An early diagnosis of trichorhinophalangeal syndrome type 1: a case report and a review of literature.Ital J Pediatr. 2018 Nov 20;44(1):138. doi: 10.1186/s13052-018-0580-z. Ital J Pediatr. 2018. PMID: 30458885 Free PMC article. Review.
-
A 45-year-old man with sudden cardiac death, cutaneous abnormalities and a rare desmoplakin mutation: a case report and literature review.BMC Cardiovasc Disord. 2022 Feb 12;22(1):41. doi: 10.1186/s12872-022-02472-5. BMC Cardiovasc Disord. 2022. PMID: 35151254 Free PMC article. Review.
References
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical