

Hyperglycaemic hyperosmolar state: first presentation of type 1 diabetes mellitus in an adolescent with complex medical needs
- PMID: 33542015
- PMCID: PMC7868183
- DOI: 10.1136/bcr-2020-237793
Hyperglycaemic hyperosmolar state: first presentation of type 1 diabetes mellitus in an adolescent with complex medical needs
Abstract
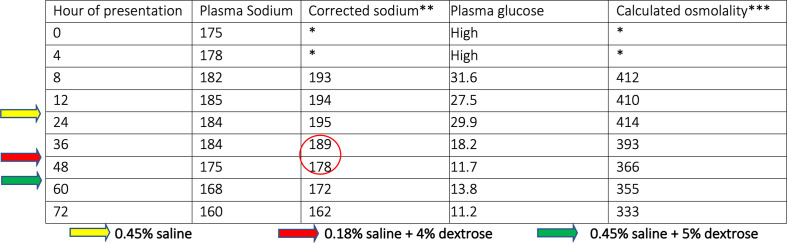
This is a case of hyperglycaemic hyperosmolar state (HHS) as first presentation of type 1 diabetes mellitus in a 14-year-old girl with background complex medical needs. She presented with marked hyperglycaemia (56 mmol/L) without significant ketonaemia (2.6 mmol/L) and serum hyperosmolality (426 mOsm/kg). Managing her profound hypernatraemic (>180 mmol/L) dehydration was challenging but resulted in good outcome. Paediatric patients with HHS will likely be treated with the diabetes ketoacidosis (DKA) protocol because of perceived rarity of HHS leading to inadequate rehydration and risk of vascular collapse. Hence, emphasis on the differences in the management protocols of DKA and HHS is paramount. Prompt recognition and adequate management are crucial to avert complications. The undesirable rate of decline of hypernatraemia due to the use of hypotonic fluid was captured in this case. We describe the pivotal role of liberal fluid therapy with non-hypotonic fluids.
Keywords: cerebral palsy; diabetes; fluid electrolyte and acid–base disturbances.
© BMJ Publishing Group Limited 2020. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Management of Hyperosmolar Hyperglycaemic State (HHS) in Adults: An updated guideline from the Joint British Diabetes Societies (JBDS) for Inpatient Care Group.Diabet Med. 2023 Mar;40(3):e15005. doi: 10.1111/dme.15005. Epub 2022 Dec 21. Diabet Med. 2023. PMID: 36370077 Free PMC article. Review.
-
Childhood diabetes presenting with hyperosmolar dehydration but without ketoacidosis: a report of three cases.Diabet Med. 2005 May;22(5):645-7. doi: 10.1111/j.1464-5491.2005.01517.x. Diabet Med. 2005. PMID: 15842523
-
Diabetic emergencies - ketoacidosis, hyperglycaemic hyperosmolar state and hypoglycaemia.Nat Rev Endocrinol. 2016 Apr;12(4):222-32. doi: 10.1038/nrendo.2016.15. Epub 2016 Feb 19. Nat Rev Endocrinol. 2016. PMID: 26893262 Review.
-
Recognizing and responding to hyperglycaemic emergencies.Br J Nurs. 2009 Oct 8-21;18(18):1094-8. doi: 10.12968/bjon.2009.18.18.44549. Br J Nurs. 2009. PMID: 19966726
-
[Hyperglycaemic crises in children and adolescents].Ned Tijdschr Geneeskd. 2013;157(50):A5185. Ned Tijdschr Geneeskd. 2013. PMID: 24326136 Review. Dutch.
Cited by
-
Hypernatremia in Hyperglycemia: Clinical Features and Relationship to Fractional Changes in Body Water and Monovalent Cations during Its Development.J Clin Med. 2024 Mar 28;13(7):1957. doi: 10.3390/jcm13071957. J Clin Med. 2024. PMID: 38610721 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical