

Increased bactericidal activity but dose-limiting intolerability at 50 mg·kg-1 rifampicin
- PMID: 33542056
- PMCID: PMC8411896
- DOI: 10.1183/13993003.00955-2020
Increased bactericidal activity but dose-limiting intolerability at 50 mg·kg-1 rifampicin
Abstract
Background: Accumulating data indicate that higher rifampicin doses are more effective and shorten tuberculosis (TB) treatment duration. This study evaluated the safety, tolerability, pharmacokinetics, and 7- and 14-day early bactericidal activity (EBA) of increasing doses of rifampicin. Here we report the results of the final cohorts of PanACEA HIGHRIF1, a dose escalation study in treatment-naive adult smear-positive patients with TB.
Methods: Patients received, in consecutive cohorts, 40 or 50 mg·kg-1 rifampicin once daily in monotherapy (day 1-7), supplemented with standard dose isoniazid, pyrazinamide and ethambutol between days 8 and 14.
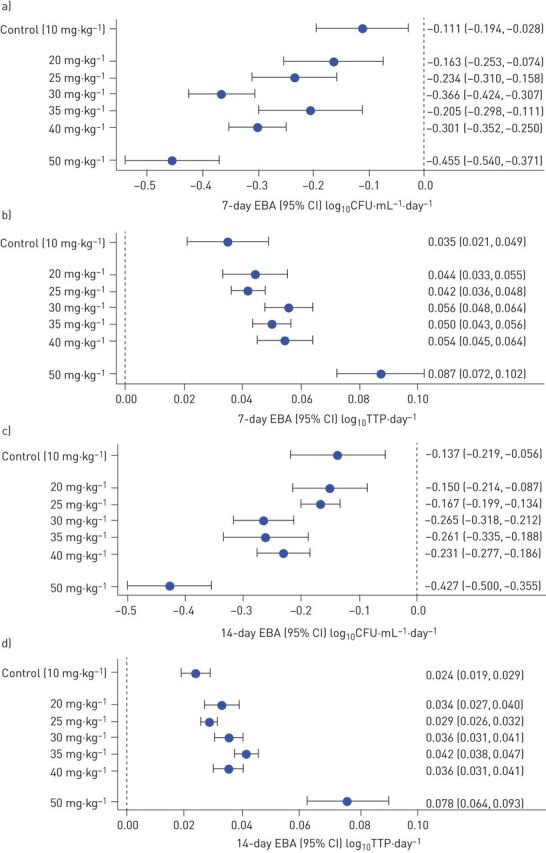
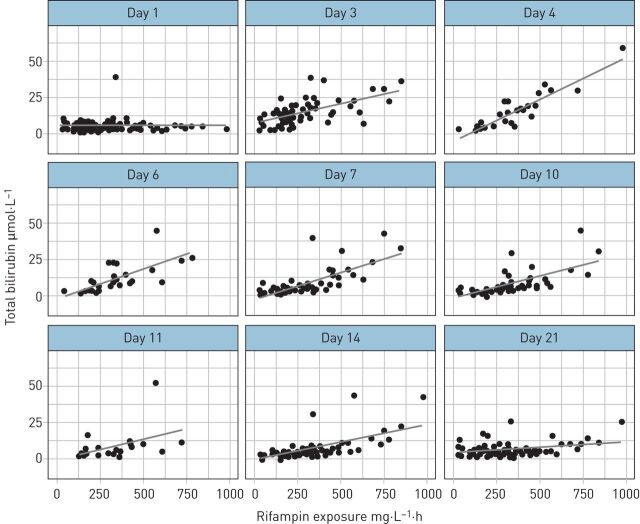
Results: In the 40 mg·kg-1 cohort (n=15), 13 patients experienced a total of 36 adverse events during monotherapy, resulting in one treatment discontinuation. In the 50 mg·kg-1 cohort (n=17), all patients experienced adverse events during monotherapy, 93 in total; 11 patients withdrew or stopped study medication. Adverse events were mostly mild/moderate and tolerability rather than safety related, i.e. gastrointestinal disorders, pruritis, hyperbilirubinaemia and jaundice. There was a more than proportional increase in the rifampicin geometric mean area under the plasma concentration-time curve from time 0 to 12 h (AUC0-24 h) for 50 mg·kg-1 compared with 40 mg·kg-1; 571 (range 320-995) versus 387 (range 201-847) mg·L-1·h, while peak exposures saw proportional increases. Protein-unbound exposure after 50 mg·kg-1 (11% (range 8-17%)) was comparable with lower rifampicin doses. Rifampicin exposures and bilirubin concentrations were correlated (Spearman's ρ=0.670 on day 3, p<0.001). EBA increased considerably with dose, with the highest seen after 50 mg·kg-1: 14-day EBA -0.427 (95% CI -0.500- -0.355) log10CFU·mL-1·day-1.
Conclusion: Although associated with an increased bactericidal effect, the 50 mg·kg-1 dose was not well tolerated. Rifampicin at 40 mg·kg-1 was well tolerated and therefore selected for evaluation in a phase IIc treatment-shortening trial.
Trial registration: ClinicalTrials.gov NCT01392911.
Copyright ©ERS 2021. For reproduction rights and permissions contact permissions@ersnet.org.
Conflict of interest statement
Conflict of interest: L.H.M. te Brake has nothing to disclose. Conflict of interest: V. de Jager has nothing to disclose. Conflict of interest: K. Narunsky has nothing to disclose. Conflict of interest: N. Vanker has nothing to disclose. Conflict of interest: E.M. Svensson has nothing to disclose. Conflict of interest: P.P.J. Phillips reports grants from Ludwig Maximilian University of Munich, during the conduct of the study. Conflict of interest: S.H. Gillespie reports grants from the European and Developing Countries Clinical Trials Partnership and TB Alliance, outside the submitted work. Conflict of interest: N. Heinrich reports grants from the European and Developing Countries Clinical Trials Partnership and German Ministry for Education and Research, during the conduct of the study; other (paid presentation) from AstraZeneca, outside the submitted work. Conflict of interest: M. Hoelscher has nothing to disclose. Conflict of interest: R. Dawson has nothing to disclose. Conflict of interest: A.H. Diacon has nothing to disclose. Conflict of interest: R.E. Aarnoutse has nothing to disclose. Conflict of interest: M.J. Boeree has nothing to disclose.
Figures

References
-
- World Health Organization . Global Tuberculosis Report 2018. Geneva, WHO, 2018.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical