

Estimated seroprevalence of SARS-CoV-2 antibodies among adults in Orange County, California
- PMID: 33542329
- PMCID: PMC7862219
- DOI: 10.1038/s41598-021-82662-x
Estimated seroprevalence of SARS-CoV-2 antibodies among adults in Orange County, California
Abstract
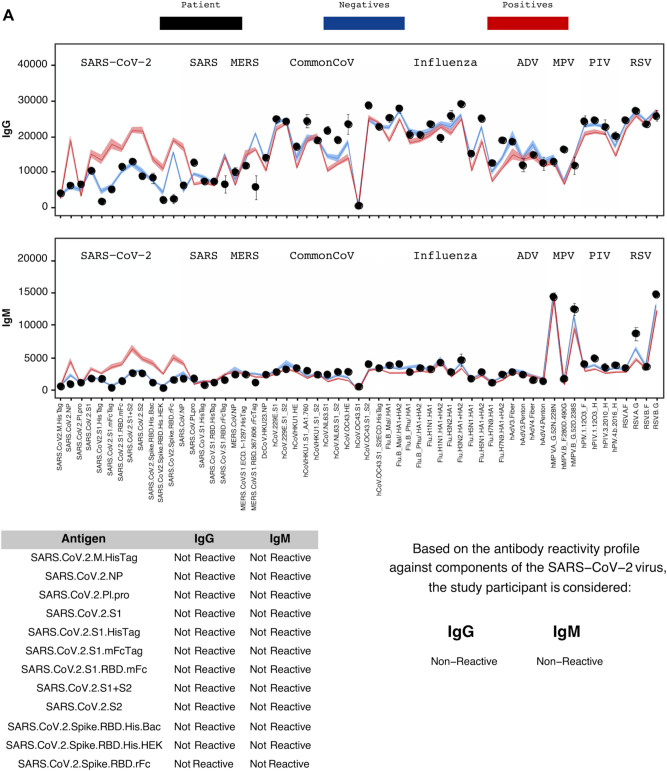
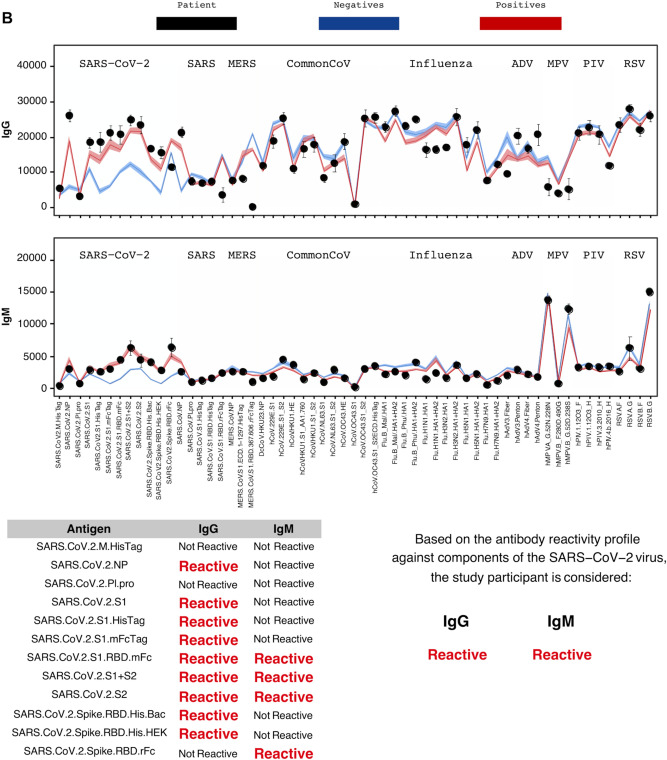
Clinic-based estimates of SARS-CoV-2 may considerably underestimate the total number of infections. Access to testing in the US has been heterogeneous and symptoms vary widely in infected persons. Public health surveillance efforts and metrics are therefore hampered by underreporting. We set out to provide a minimally biased estimate of SARS-CoV-2 seroprevalence among adults for a large and diverse county (Orange County, CA, population 3.2 million). We implemented a surveillance study that minimizes response bias by recruiting adults to answer a survey without knowledge of later being offered SARS-CoV-2 test. Several methodologies were used to retrieve a population-representative sample. Participants (n = 2979) visited one of 11 drive-thru test sites from July 10th to August 16th, 2020 (or received an in-home visit) to provide a finger pin-prick sample. We applied a robust SARS-CoV-2 Antigen Microarray technology, which has superior measurement validity relative to FDA-approved tests. Participants include a broad age, gender, racial/ethnic, and income representation. Adjusted seroprevalence of SARS-CoV-2 infection was 11.5% (95% CI: 10.5-12.4%). Formal bias analyses produced similar results. Prevalence was elevated among Hispanics (vs. other non-Hispanic: prevalence ratio [PR] = 1.47, 95% CI 1.22-1.78) and household income < $50,000 (vs. > $100,000: PR = 1.42, 95% CI: 1.14 to 1.79). Results from a diverse population using a highly specific and sensitive microarray indicate a SARS-CoV-2 seroprevalence of ~ 12 percent. This population-based seroprevalence is seven-fold greater than that using official County statistics. In this region, SARS-CoV-2 also disproportionately affects Hispanic and low-income adults.
Conflict of interest statement
Dr. Saahir Khan reports grants from University of California Office of the President and from National Institutes of Health during the conduct of the study. In addition, Dr. Khan has a patent “Devices For Detecting Antibodies To Coronavirus Antigens And Methods for Using Them,” Provisional Patent No. 62/993,610, filed March 23, 2020, licensed to Nanommune Inc. Saahir Khan is a consultant for and owns shares in Nanommune Inc. which is commercializing the technology used in this study. All other Authors (Drs. Bruckner, Parker, Bartell, Vieira, Drum, Noymer, Albala, Boden-Albala, Zahn) declare no potential conflict of interest.
Figures
References
-
- Thacker SB. Historical Development. In: Teutsch SM, Churchill RE, editors. Principles and Practice of Public Health Surveillance. New York: Oxford University Press; 2000. pp. 1–16.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
