

Saliva is more sensitive than nasopharyngeal or nasal swabs for diagnosis of asymptomatic and mild COVID-19 infection
- PMID: 33542443
- PMCID: PMC7862309
- DOI: 10.1038/s41598-021-82787-z
Saliva is more sensitive than nasopharyngeal or nasal swabs for diagnosis of asymptomatic and mild COVID-19 infection
Erratum in
-
Author Correction: Saliva is more sensitive than nasopharyngeal or nasal swabs for diagnosis of asymptomatic and mild COVID-19 infection.Sci Rep. 2021 Jun 9;11(1):12538. doi: 10.1038/s41598-021-89880-3. Sci Rep. 2021. PMID: 34108515 Free PMC article. No abstract available.
Abstract
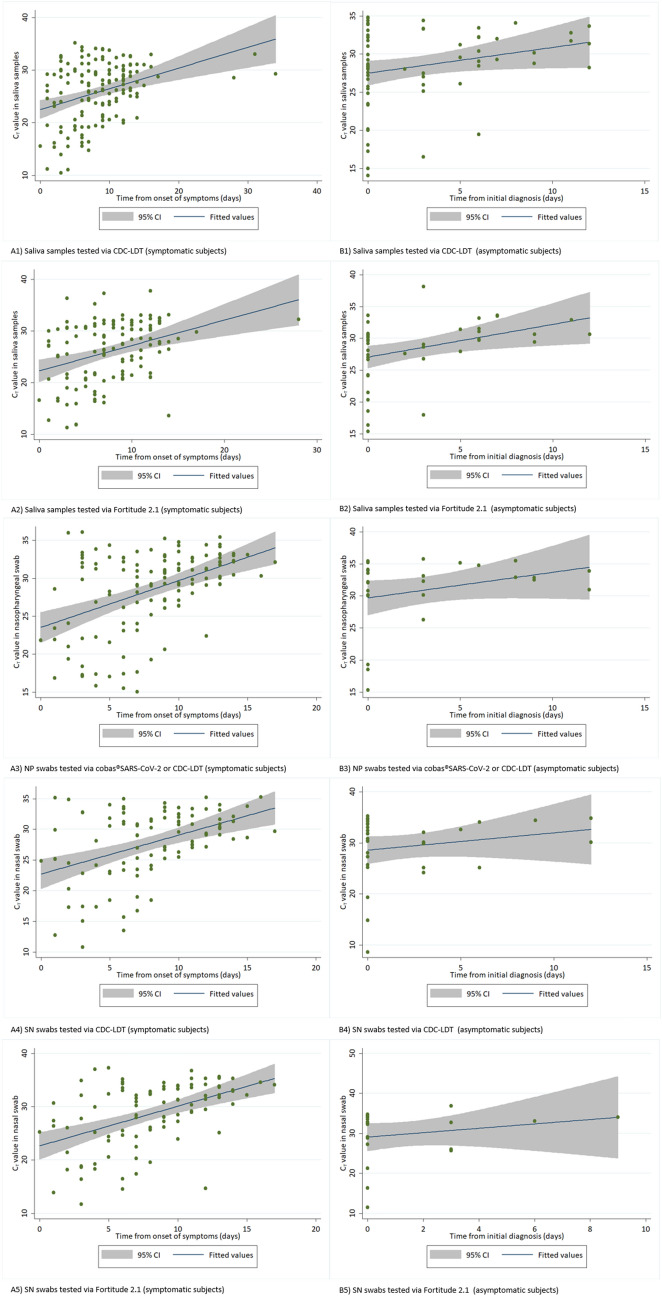
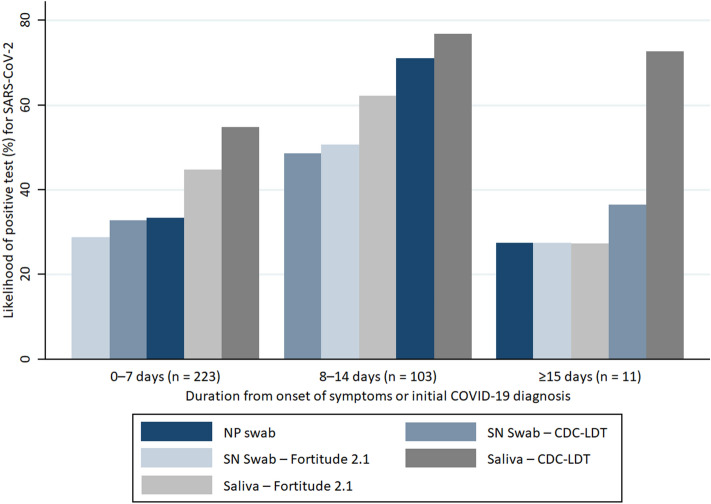
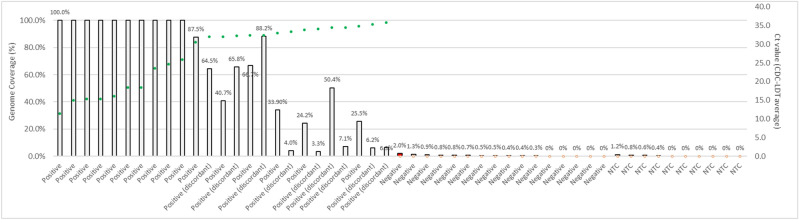
We aimed to test the sensitivity of naso-oropharyngeal saliva and self-administered nasal (SN) swab compared to nasopharyngeal (NP) swab for COVID-19 testing in a large cohort of migrant workers in Singapore. We also tested the utility of next-generation sequencing (NGS) for diagnosis of COVID-19. Saliva, NP and SN swabs were collected from subjects who presented with acute respiratory infection, their asymptomatic roommates, and prior confirmed cases who were undergoing isolation at a community care facility in June 2020. All samples were tested using RT-PCR. SARS-CoV-2 amplicon-based NGS with phylogenetic analysis was done for 30 samples. We recruited 200 subjects, of which 91 and 46 were tested twice and thrice respectively. In total, 62.0%, 44.5%, and 37.7% of saliva, NP and SN samples were positive. Cycle threshold (Ct) values were lower during the earlier period of infection across all sample types. The percentage of test-positive saliva was higher than NP and SN swabs. We found a strong correlation between viral genome coverage by NGS and Ct values for SARS-CoV-2. Phylogenetic analyses revealed Clade O and lineage B.6 known to be circulating in Singapore. We found saliva to be a sensitive and viable sample for COVID-19 diagnosis.
Conflict of interest statement
Yukti Choudhury, Chae Yin Cher, Zi Yi Wan, and Min Han Tan are employees of, and affiliated with, Lucence. Y.C. and M.H.T. are shareholders of Lucence; M.H.T. is a director of Lucence. An affiliated entity of Lucence is the applicant of certain patent applications for relevant diagnostics. Y.C., C.Y.C. and/or M.H.T. are named inventors for some of these patent applications. At the time of this research, patents are pending for the next-generation sequencing approach (SG App. No. 10202007270P) and the saliva testing process (SG App. No. 10202007826S) discussed in the manuscript.
Figures
References
-
- World Health Organization. Novel Coronavirus (2019-nCoV) Situation Report (2020). https://www.who.int/docs/default-source/coronaviruse/situation-reports/2.... Accessed 1 September 2020.
-
- Worldometer. COVID-19 Coronavirus Pandemic (2020). https://www.worldometers.info/coronavirus/#countries. Accessed 1 September 2020.
-
- Ministry of Health Singapore. COVID-19 Situation Report (2020). https://covidsitrep.moh.gov.sg/. Accessed 1 September 2020.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
