

Prevalence of posttraumatic stress disorder after infectious disease pandemics in the twenty-first century, including COVID-19: a meta-analysis and systematic review
- PMID: 33542468
- PMCID: PMC7861006
- DOI: 10.1038/s41380-021-01036-x
Prevalence of posttraumatic stress disorder after infectious disease pandemics in the twenty-first century, including COVID-19: a meta-analysis and systematic review
Abstract
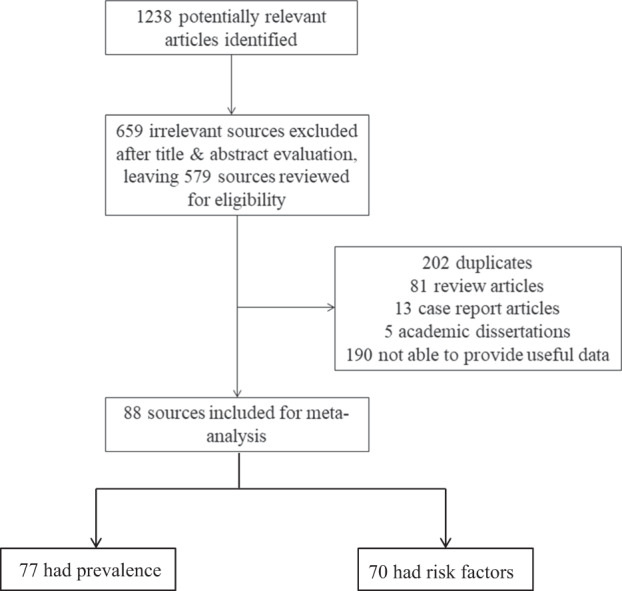
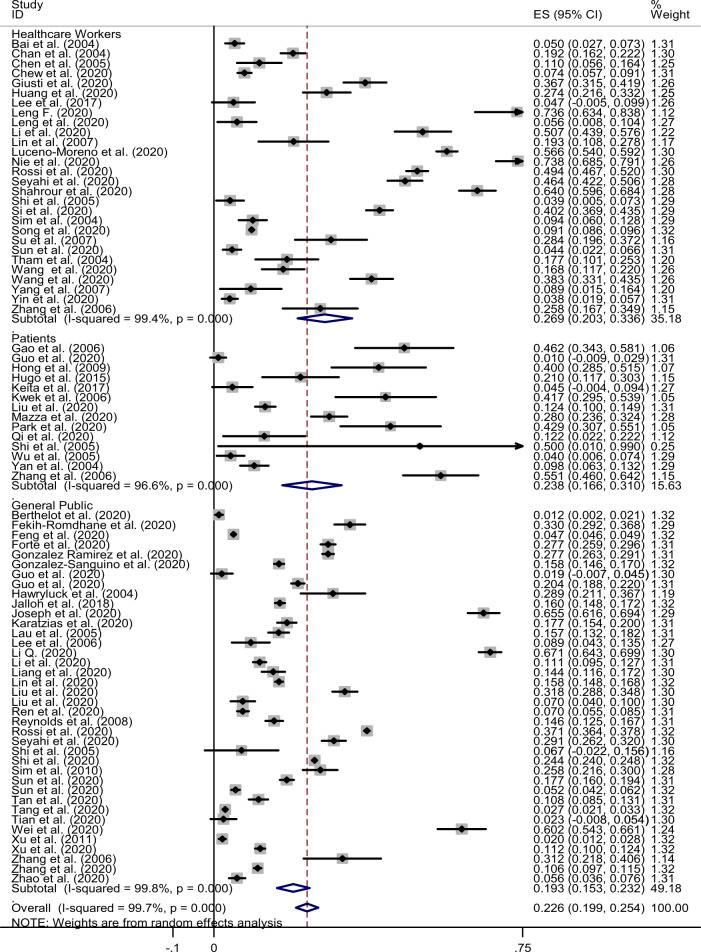
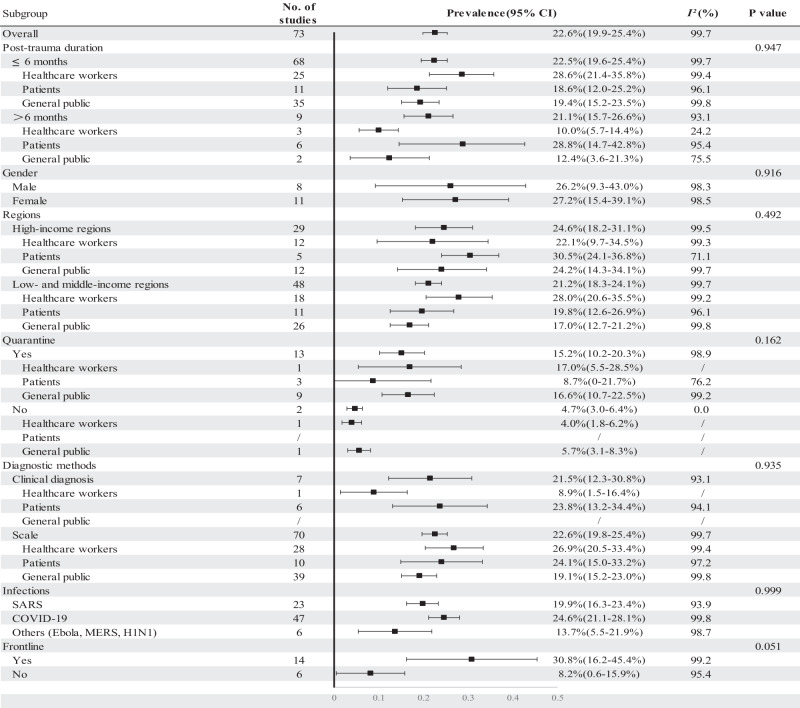
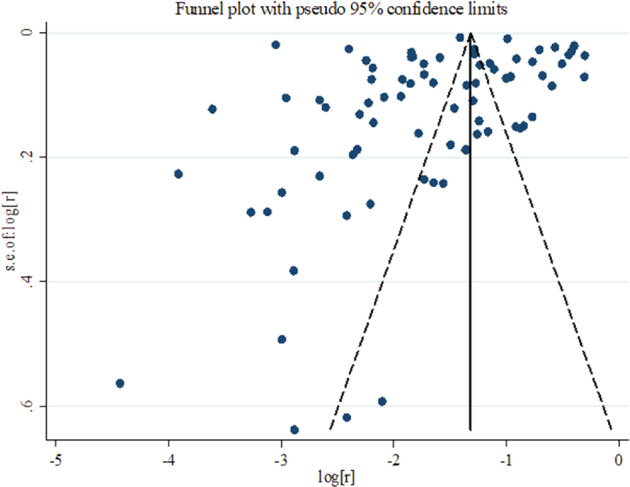
Pandemics have become more frequent and more complex during the twenty-first century. Posttraumatic stress disorder (PTSD) following pandemics is a significant public health concern. We sought to provide a reliable estimate of the worldwide prevalence of PTSD after large-scale pandemics as well as associated risk factors, by a systematic review and meta-analysis. We systematically searched the MedLine, Embase, PsycINFO, Web of Science, CNKI, WanFang, medRxiv, and bioRxiv databases to identify studies that were published from the inception up to August 23, 2020, and reported the prevalence of PTSD after pandemics including sudden acute respiratory syndrome (SARS), H1N1, Poliomyelitis, Ebola, Zika, Nipah, Middle Eastern respiratory syndrome coronavirus (MERS-CoV), H5N1, and coronavirus disease 2019 (COVID-19). A total of 88 studies were included in the analysis, with 77 having prevalence information and 70 having risk factors information. The overall pooled prevalence of post-pandemic PTSD across all populations was 22.6% (95% confidence interval (CI): 19.9-25.4%, I2: 99.7%). Healthcare workers had the highest prevalence of PTSD (26.9%; 95% CI: 20.3-33.6%), followed by infected cases (23.8%: 16.6-31.0%), and the general public (19.3%: 15.3-23.2%). However, the heterogeneity of study findings indicates that results should be interpreted cautiously. Risk factors including individual, family, and societal factors, pandemic-related factors, and specific factors in healthcare workers and patients for post-pandemic PTSD were summarized and discussed in this systematic review. Long-term monitoring and early interventions should be implemented to improve post-pandemic mental health and long-term recovery.
© 2021. The Author(s), under exclusive licence to Springer Nature Limited part of Springer Nature.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Madhav N, Oppenheim B, Gallivan M, Mulembakani P, Rubin E, Wolfe N. Pandemics: risks, impacts, and mitigation. Washington, DC: The International Bank for Reconstruction and Development/The World Bank; 2017. 10.1596/978-1-4648-0527-1/pt5.ch17. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
