

Predicting COVID-19 mortality with electronic medical records
- PMID: 33542473
- PMCID: PMC7862405
- DOI: 10.1038/s41746-021-00383-x
Predicting COVID-19 mortality with electronic medical records
Abstract
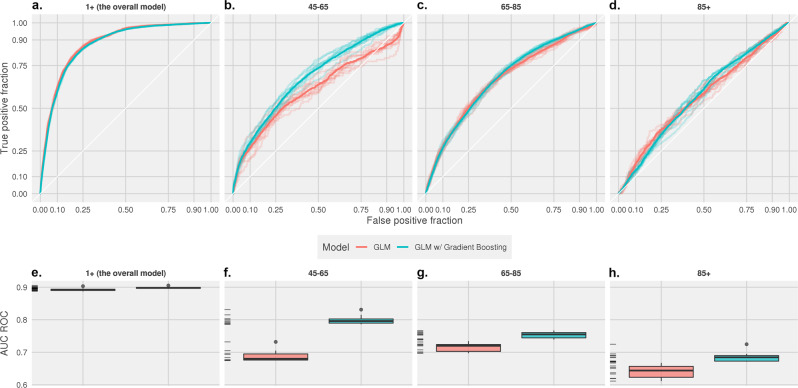
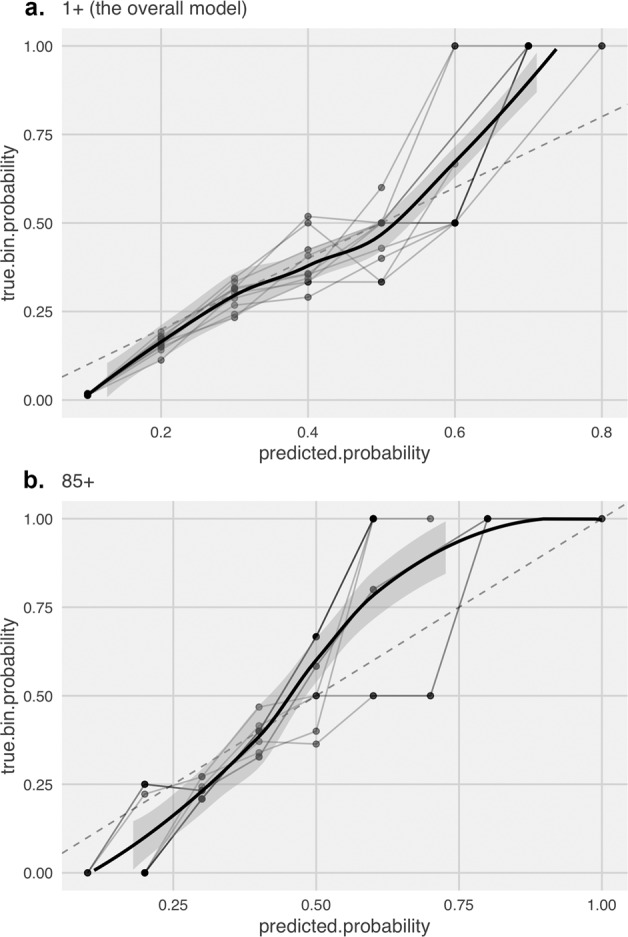
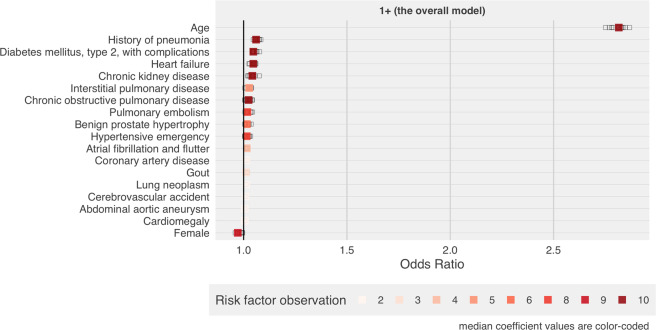
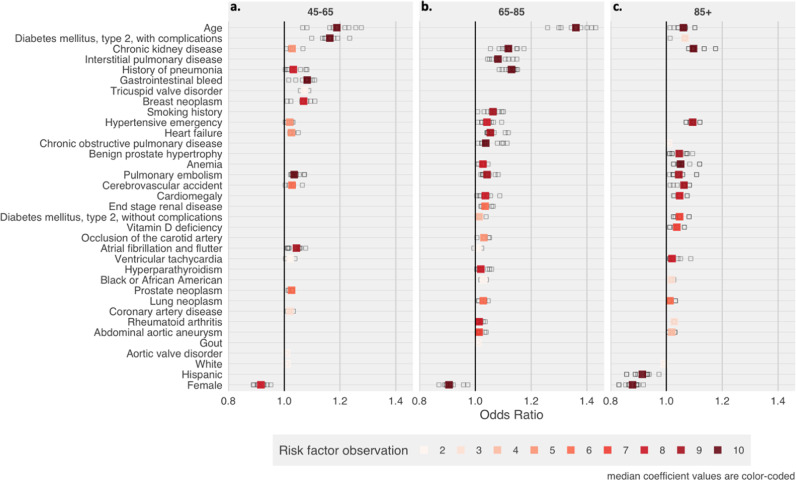
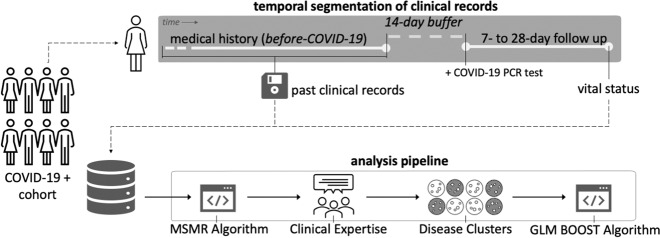
This study aims to predict death after COVID-19 using only the past medical information routinely collected in electronic health records (EHRs) and to understand the differences in risk factors across age groups. Combining computational methods and clinical expertise, we curated clusters that represent 46 clinical conditions as potential risk factors for death after a COVID-19 infection. We trained age-stratified generalized linear models (GLMs) with component-wise gradient boosting to predict the probability of death based on what we know from the patients before they contracted the virus. Despite only relying on previously documented demographics and comorbidities, our models demonstrated similar performance to other prognostic models that require an assortment of symptoms, laboratory values, and images at the time of diagnosis or during the course of the illness. In general, we found age as the most important predictor of mortality in COVID-19 patients. A history of pneumonia, which is rarely asked in typical epidemiology studies, was one of the most important risk factors for predicting COVID-19 mortality. A history of diabetes with complications and cancer (breast and prostate) were notable risk factors for patients between the ages of 45 and 65 years. In patients aged 65-85 years, diseases that affect the pulmonary system, including interstitial lung disease, chronic obstructive pulmonary disease, lung cancer, and a smoking history, were important for predicting mortality. The ability to compute precise individual-level risk scores exclusively based on the EHR is crucial for effectively allocating and distributing resources, such as prioritizing vaccination among the general population.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- NYC Health. City of New York. COVID-19: Data. https://www1.nyc.gov/site/doh/covid/covid-19-data.page (2020).
Grants and funding
- R01 HG009174/HG/NHGRI NIH HHS/United States
- T15 LM007092/LM/NLM NIH HHS/United States
- R01-HG009174/U.S. Department of Health & Human Services | NIH | National Human Genome Research Institute (NHGRI)
- T15LM007092/U.S. Department of Health & Human Services | NIH | U.S. National Library of Medicine (NLM)
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
