

Tapentadol for the Treatment of Moderate-to-Severe Acute Pain in Children Under the Age of Two Years
- PMID: 33542653
- PMCID: PMC7853441
- DOI: 10.2147/JPR.S269530
Tapentadol for the Treatment of Moderate-to-Severe Acute Pain in Children Under the Age of Two Years
Abstract
Background: Pharmacokinetics (PK), efficacy, and safety of the opioid analgesic tapentadol in the treatment of moderate-to-severe acute pain have so far not been investigated in pediatric patients <2 years of age.
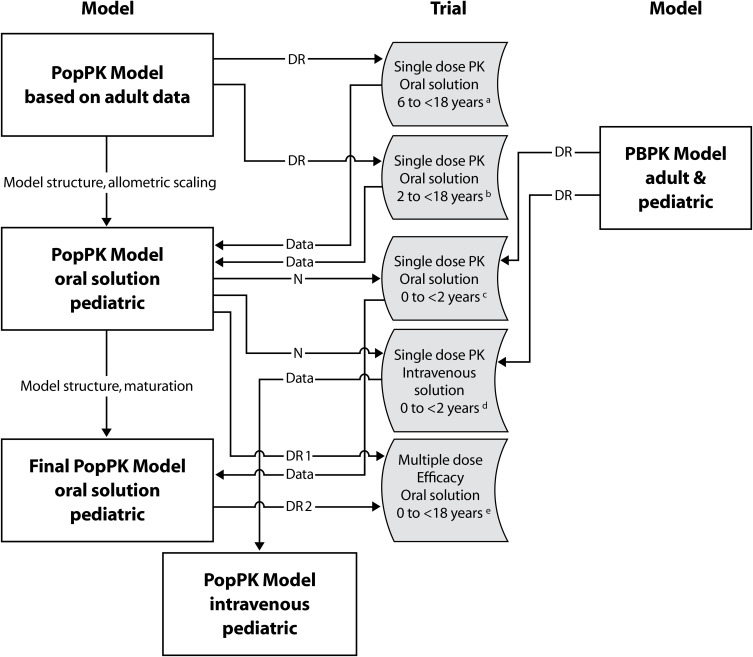
Patients and methods: Two multicenter, open-label trials assessed the pharmacokinetic profile, safety, tolerability, and efficacy of single doses of tapentadol oral solution (OS; NCT02221674; n=19) or intravenous infusion (IV, EudraCT 2014-002259-24; n=38) in children from birth to <2 years of age. Of these, 8 preterm neonates were included in the IV trial. A third randomized, double-blind, placebo-controlled trial (NCT02081391) investigated the efficacy and safety of multiple tapentadol OS doses in patients from birth to <2 years (placebo n=4, tapentadol n=11) using an immediate rescue trial design. Patients in all three trials underwent surgery that, in the investigator's opinion, reliably produced moderate-to-severe pain requiring opioid treatment.
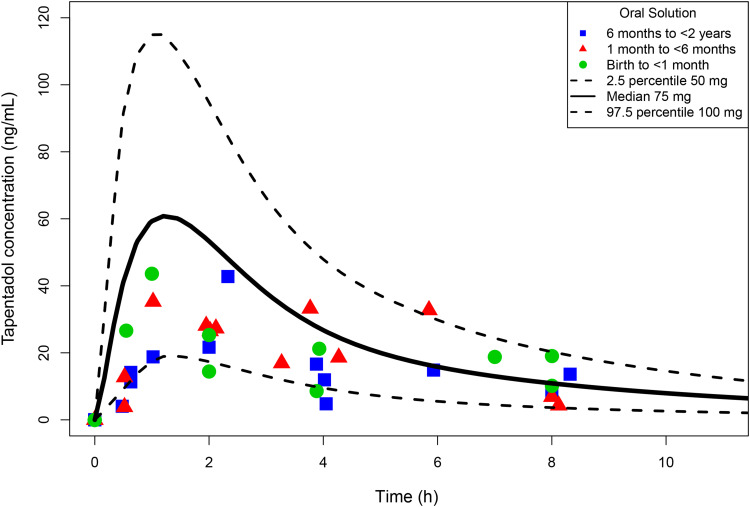
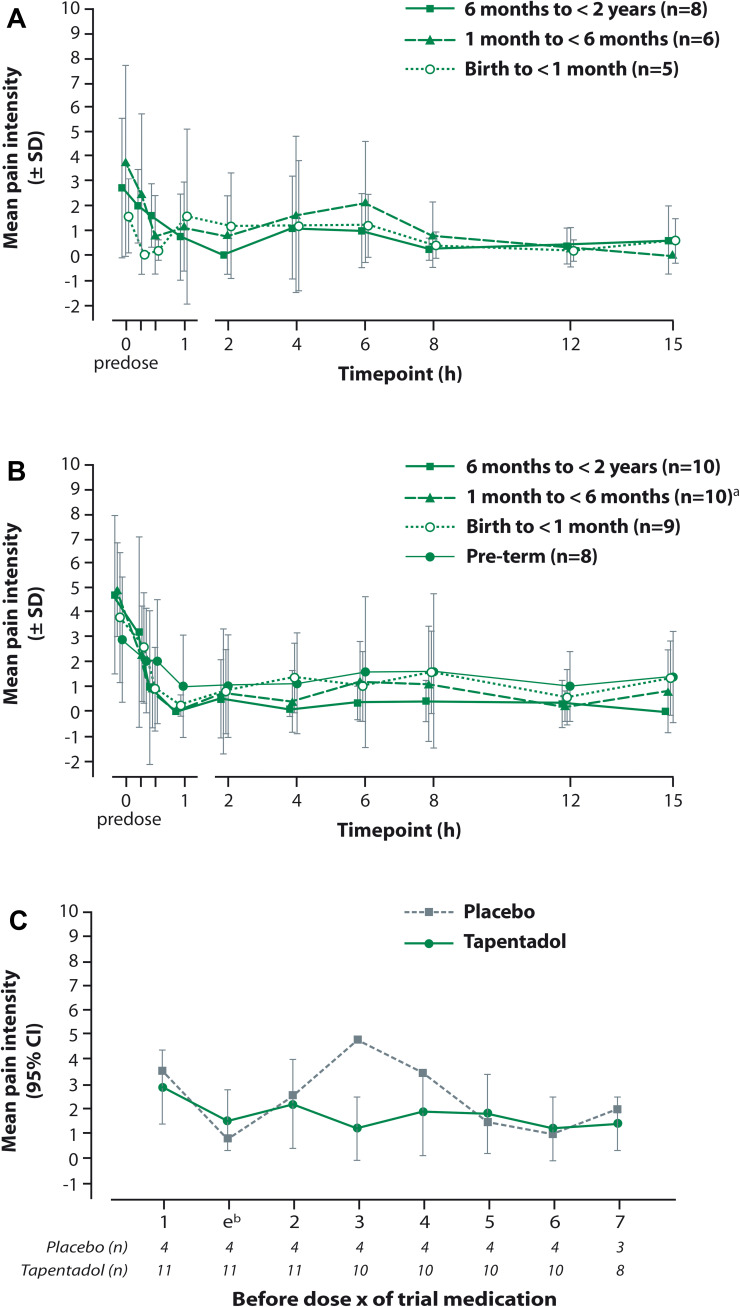
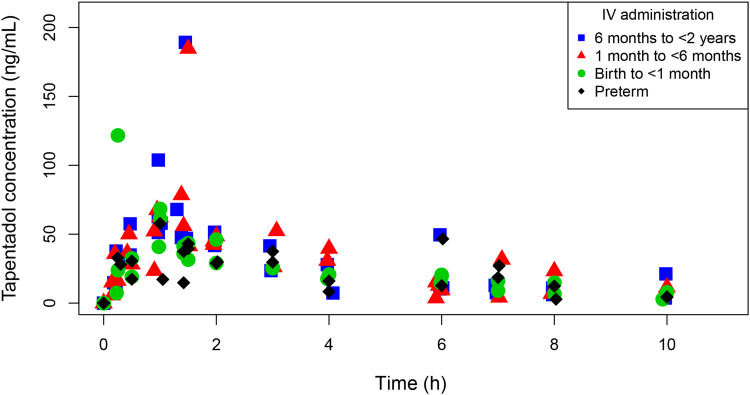
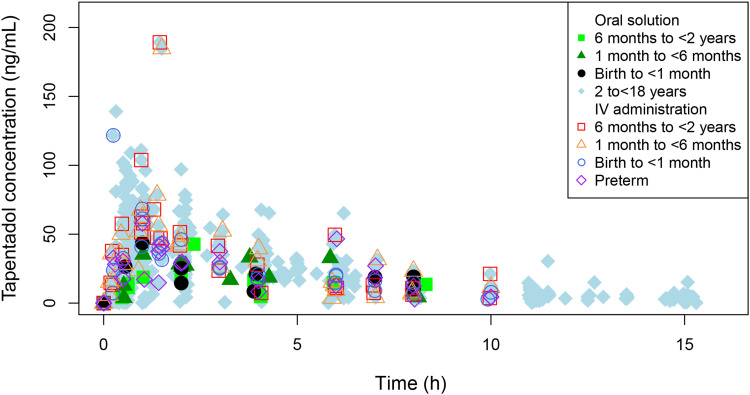
Results: Administration of single tapentadol doses resulted in tapentadol serum concentrations within the targeted range known to be safe and efficacious in adults and compared well to the range observed for children aged 2 to <18 years. Pain intensity already improved 15 min after administration. In the multiple dose trial, amounts of supplemental opioid analgesic medication within the first 24 h after start of trial medication were low (placebo 0.02 mg/kg, tapentadol 0.05 mg/kg). All patients stopped treatment with the trial medication because opioid analgesics were no longer required. Treatment-emergent adverse events occurred in 42.1% (tapentadol OS single dose), 28.9% (tapentadol IV), and 75% of placebo and 54.5% of tapentadol patients (tapentadol OS multiple doses), none of them serious.
Conclusion: Tapentadol showed a favorable PK and safety profile in children <2 years of age. Multiple tapentadol OS dosing is efficacious and generally well tolerated in children ≥2 years and might also be a useful treatment option for children <2 years in need of strong analgesics.
Keywords: infants; intravenous formulation; neonates; oral formulation; pain management; tapentadol.
© 2021 Eissa et al.
Conflict of interest statement
AE and GBH were investigators on the clinical trials published here and were paid by Grünenthal GmbH for their contributions to these trials. ET was an employee of Grünenthal USA Inc. at the time the trials were conducted. EW was an employee of Grünenthal GmbH at the time the trials were conducted. All other authors are current employees of Grünenthal GmbH. The authors report no other potential conflicts of interest for this work.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
