

Bone lesions on baseline staging rectal MRI: prevalence and significance in patients with rectal adenocarcinoma
- PMID: 33543320
- PMCID: PMC9309895
- DOI: 10.1007/s00261-020-02923-7
Bone lesions on baseline staging rectal MRI: prevalence and significance in patients with rectal adenocarcinoma
Erratum in
-
Correction to: Bone lesions on baseline staging rectal MRI: prevalence and significance in patients with rectal adenocarcinoma.Abdom Radiol (NY). 2021 Jun;46(6):2432. doi: 10.1007/s00261-021-03012-z. Abdom Radiol (NY). 2021. PMID: 33742219 Free PMC article. No abstract available.
Abstract
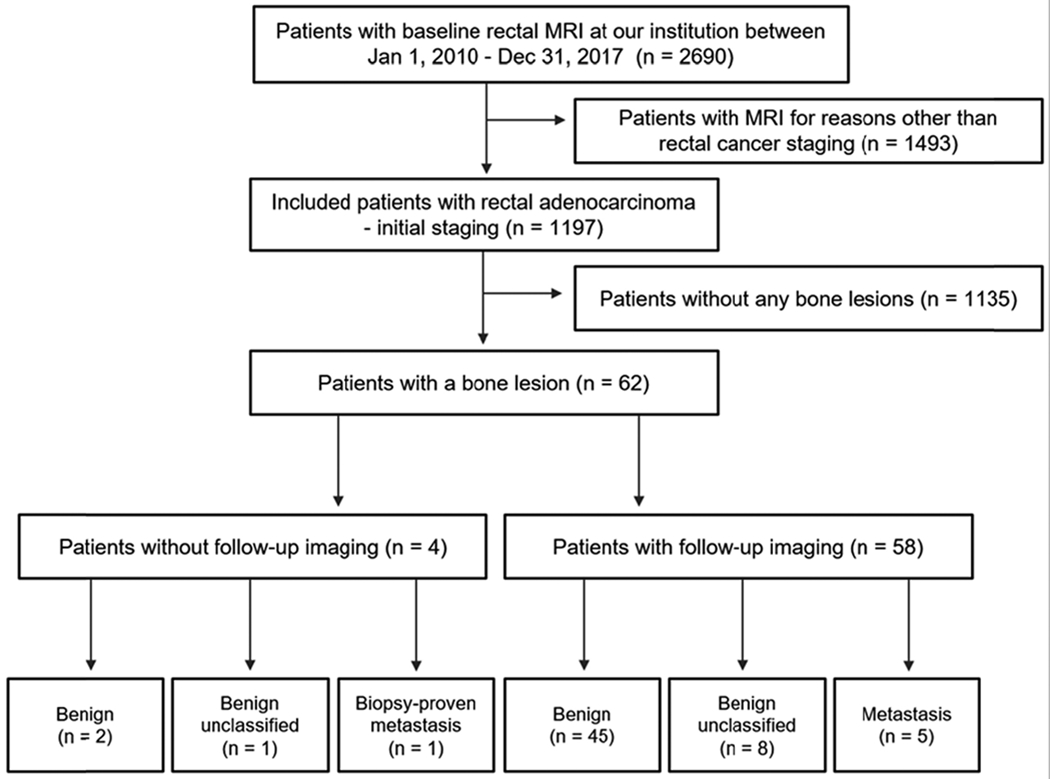
A T1 sequence on routine baseline staging rectal magnetic resonance imaging (MRI) is thought to help detect bone lesions. Our primary aim was to evaluate the incidence of bone lesions encountered on baseline staging rectal MRI, particularly the prevalence of bone metastases. This retrospective study included patients with rectal adenocarcinoma who underwent baseline rectal MRI at our institution between January 2010 and December 2017. The MRI report was reviewed for presence of bone lesions. When found, lesion type, presence of axial T1 non-fat-suppressed sequence, primary tumor T-stage, and presence of other organ metastases were recorded. In the absence of bone biopsy, the reference standard was follow-up imaging via computed tomography (CT), MRI, and/or positron emission tomography/CT (PET/CT) ≥ 1 year after the baseline MRI. The Wilcoxon rank-sum test and Fisher's exact test were used to compare clinicopathologic data of patients with malignant or benign bone lesions. A total of 1197 patients were included. 62/1197 patients (mean age 56.8 years (SD: 13.8), with 39 men) had bone lesions on baseline imaging, with 6 being bone metastases (0.5%, 95% CI 0.2%-1.1%). Of the 6 patients with bone metastases, 5/6 had other metastases (i.e., liver, lung) at baseline. Bone metastases on baseline rectal MRI performed for rectal adenocarcinoma are extremely rare. Furthermore, bone metastases without other organ (i.e., liver, lung) involvement is extremely rare.
Keywords: Bone neoplasm; Magnetic resonance imaging; Rectal neoplasm.
Conflict of interest statement
Figures
References
-
- Meyer JE, Narang T, Schnoll-Sussman FH, Pochapin MB, Christos PJ, Sherr DL (2010) Increasing incidence of rectal cancer in patients aged younger than 40 years: an analysis of the surveillance, epidemiology, and end results database. Cancer 116 (18):4354–4359. doi: 10.1002/cncr.25432 - DOI - PMC - PubMed
-
- Norenberg D, Sommer WH, Thasler W, D’Haese J, Rentsch M, Kolben T, Schreyer A, Rist C, Reiser M, Armbruster M (2017) Structured Reporting of Rectal Magnetic Resonance Imaging in Suspected Primary Rectal Cancer: Potential Benefits for Surgical Planning and Interdisciplinary Communication. Invest Radiol 52 (4):232–239. doi: 10.1097/RLI.0000000000000336 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
