

Effects of sarcopenia and malnutrition on morbidity and mortality in gynecologic cancer surgery: results of a prospective study
- PMID: 33543597
- PMCID: PMC8061344
- DOI: 10.1002/jcsm.12676
Effects of sarcopenia and malnutrition on morbidity and mortality in gynecologic cancer surgery: results of a prospective study
Abstract
Background: Malnutrition and sarcopenia often occur simultaneously in cancer patients and are thought to have harmful effects on both surgical and oncological outcomes. Therefore, we want to evaluate the effects of sarcopenia and malnutrition on severe postoperative complications and overall survival in gynecologic cancer patients.
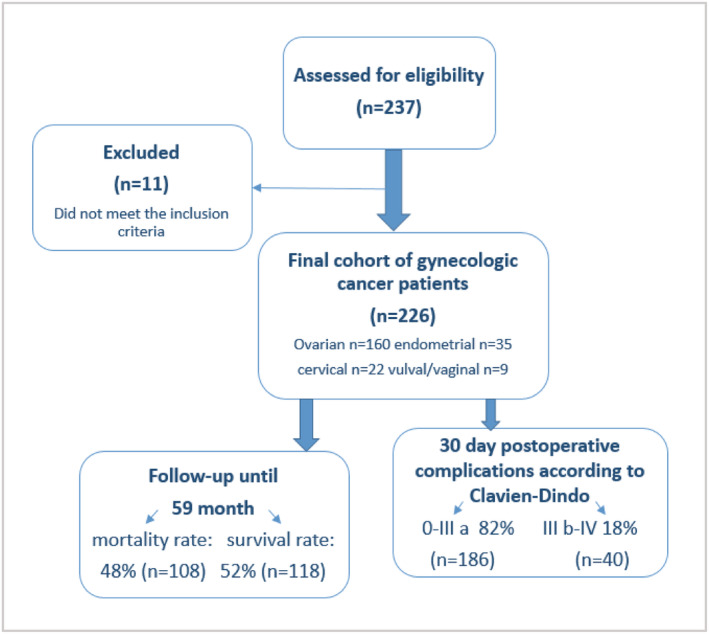
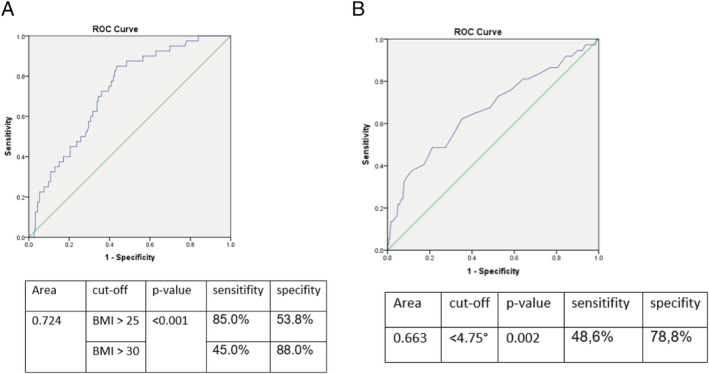
Methods: We assessed nutritional parameters and run a bioelectrical impedance analysis in 226 women. Extracellular mass to body cell mass index, phase angle alpha, muscle mass, and fat mass were evaluated. To determine if patients suffer from sarcopenia, we ran the Timed 'Up and Go' test, performed hand grip strength, and calculated a skeletal muscle index. Postoperative complications were categorized using Clavien-Dindo Classification. Utilizing ROC analysis and logistic regression, we determined predictive clinical factors for severe postoperative complications. Kaplan-Meier method and log-rank test were used for overall survival analysis.
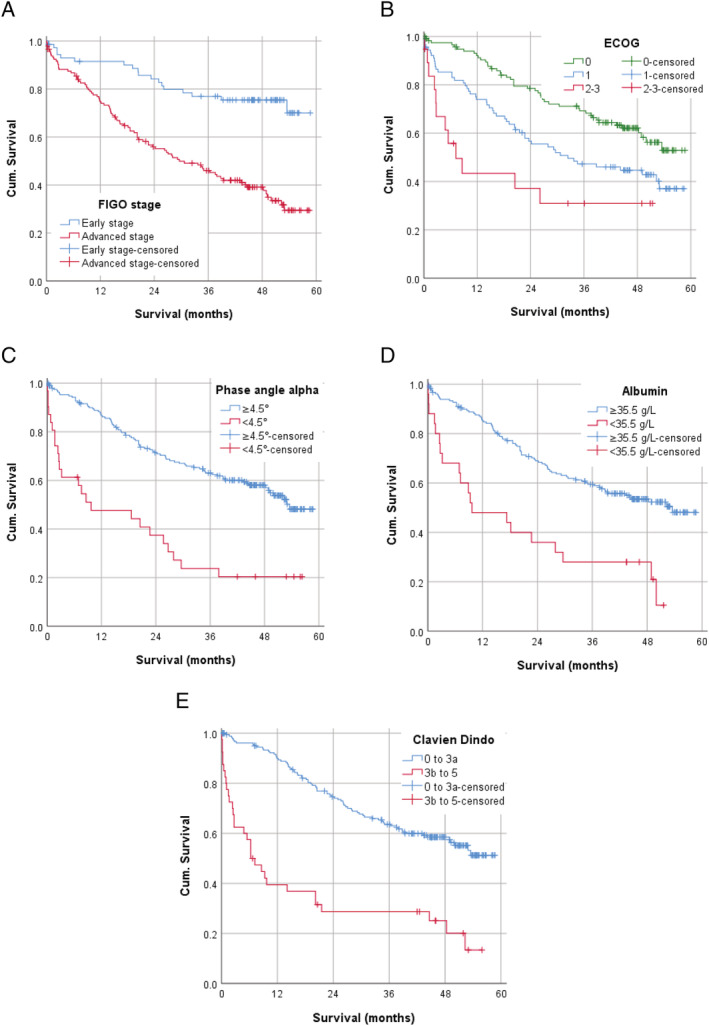
Results: Of the 226 female patients, 120 (53%) had a BMI ≥ 25 kg/m2 , 56 (26%) had a phase angle < 4.75°, and 68 (32%) were sarcopenic according to skeletal muscle index < 27%. Within 30 days after surgery, 40 (18%) patients developed severe postoperative complications, and 4% had died. According to multivariable regression analysis, ECOG status > 1 (OR 4.56, 95% CI: 1.46-14.28, P = 0.009), BMI ≥ 25 kg/m2 (OR 8.22, 95% CI: 3.01-22.48, P < 0.001), phase angle < 4.75° (OR 3.95, 95% CI: 1.71-9.10, P = 0.001), and tumour stage ≥ III A (OR 3.65, 95% CI: 1.36-9.76, P = 0.01) were predictors of severe postoperative complications. During 59 months of follow-up, 108 (48%) patients had died. According to multivariable Cox regression ECOG status > 1 (HR 2.51, 95% CI: 1.25-5.03, P = 0.01), hypoalbuminemia (HR 2.15, 95% CI: 1.28-3.59, P = 0.004), phase angle < 4.5° (HR 1.76, 95% CI 1.07-2.90, P = 0.03), tumour stage ≥ III A (HR 2.61, 95% CI: 1.53-4.45, P < 0.001), and severe postoperative complications (HR 2.82, 95% CI: 1.80-4.41, P < 0.001) were predictors of overall mortality.
Conclusions: We observed that preoperatively assessed ECOG status > 1, BMI > 25 kg, as well as phase angle alpha < 4.75° and FIGO stage ≥ III A are significantly associated with severe postoperative complications within the first month. Whereas ECOG status > 1, hypoalbuminemia, phase angle < 4.5° as well as FIGO stage ≥ III A and severe postoperative complications within 30 days correlate significantly with poor overall survival.
Keywords: Gynecologic oncology; Malnutrition; Overall survival; Postoperative complications; Sarcopenia.
© 2021 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of Society on Sarcopenia, Cachexia and Wasting Disorders.
Conflict of interest statement
Dr. Anker reports personal fees from Servier, outside the submitted work. All other authors declare no conflict of interest.
Figures
References
-
- Romeo A, Gonzalez MI, Jaunarena J, Zubieta ME, Favre G, Tejerizo JC. Pelvic exenteration for gynecologic malignancies: postoperative complications and oncologic outcomes. Actas Urol Esp 2018;42:121–125. - PubMed
-
- Otten L, Stobäus N, Franz K, Genton L, Müller‐Werdan U, Wirth R, et al. Impact of sarcopenia on 1‐year mortality in older patients with cancer. Age Ageing 2019;48:413–418. - PubMed
-
- Reisinger KW, van Vugt JLA, Tegels JJW, Snijders C, Hulsewé KW, Hoofwijk AG, et al. Functional compromise reflected by sarcopenia, frailty, and nutritional depletion predicts adverse postoperative outcome after colorectal cancer surgery. Ann Surg 2015;261:345–352. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
