

How to Treat Peripheral Arteriovenous Malformations
- PMID: 33543847
- PMCID: PMC8005356
- DOI: 10.3348/kjr.2020.0981
How to Treat Peripheral Arteriovenous Malformations
Abstract
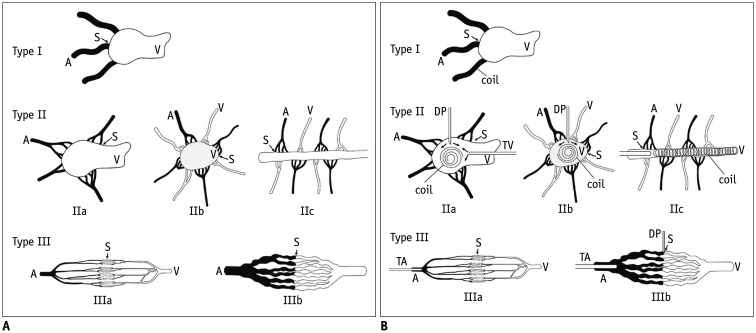
Arteriovenous malformations (AVMs) are direct communications between primitive reticular networks of dysplastic vessels that have failed to mature into capillary vessels. Based on angiographic findings, peripheral AVMs can be classified into six types: type I, type IIa, type IIb, type IIc, type IIIa, and type IIIb. Treatment strategies vary with the types. Type I is treated by embolizing the fistula between the artery and the vein with coils. Type II (IIa, IIb, and IIc) AVM is treated as follows: first, reduce the blood flow velocity in the venous segment of the AVM with coils; second, perform ethanol embolotherapy of the residual shunts. Type IIIa is treated by transarterial catheterization of the feeding arteries and injection of diluted ethanol. Type IIIb is treated by transarterial or direct puncture approaches. A high concentration of ethanol is injected through the transarterial catheter or direct puncture needle. When the fistula is large, coil insertion is required to reduce the amount of ethanol. Type I and type II AVMs showed the best clinical results; type IIIb showed a satisfactory response rate. However, type IIIa showed the poorest response rate, either alone or in combination with other types. Clinical success can be achieved by using different treatment strategies for different angiographic AVM types.
Keywords: Angiography; Arteriovenous malformation; Embolotherapy.
Copyright © 2021 The Korean Society of Radiology.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures






References
-
- Lee BB, Baumgartner I, Berlien HP, Bianchini G, Burrows P, Do YS, et al. Consensus document of the international union of angiology (IUA)-2013. Current concept on the management of arterio-venous malformations. Int Angiol. 2013;32:9–36. - PubMed
-
- Park HS, Do YS, Park KB, Kim DI, Kim YW, Kim MJ, et al. Ethanol embolotherapy of hand arteriovenous malformations. J Vasc Surg. 2011;53:725–731. - PubMed
-
- Do YS, Kim YW, Park KB, Kim DI, Park HS, Cho SK, et al. Endovascular treatment combined with embolosclerotherapy for pelvic arteriovenous malformations. J Vasc Surg. 2012;55:465–471. - PubMed
-
- Cho SK, Do YS, Shin SW, Kim DI, Kim YW, Park KB, et al. Arteriovenous malformations of the body and extremities: analysis of therapeutic outcomes and approaches according to a modified angiographic classification. J Endovasc Ther. 2006;13:527–538. - PubMed
-
- Flye MW, Jordan BP, Schwartz MZ. Management of congenital arteriovenous malformations. Surgery. 1983;94:740–747. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
