

COVID-19 versus Non-COVID-19 Acute Respiratory Distress Syndrome: Comparison of Demographics, Physiologic Parameters, Inflammatory Biomarkers, and Clinical Outcomes
- PMID: 33544045
- PMCID: PMC8328355
- DOI: 10.1513/AnnalsATS.202008-1026OC
COVID-19 versus Non-COVID-19 Acute Respiratory Distress Syndrome: Comparison of Demographics, Physiologic Parameters, Inflammatory Biomarkers, and Clinical Outcomes
Abstract
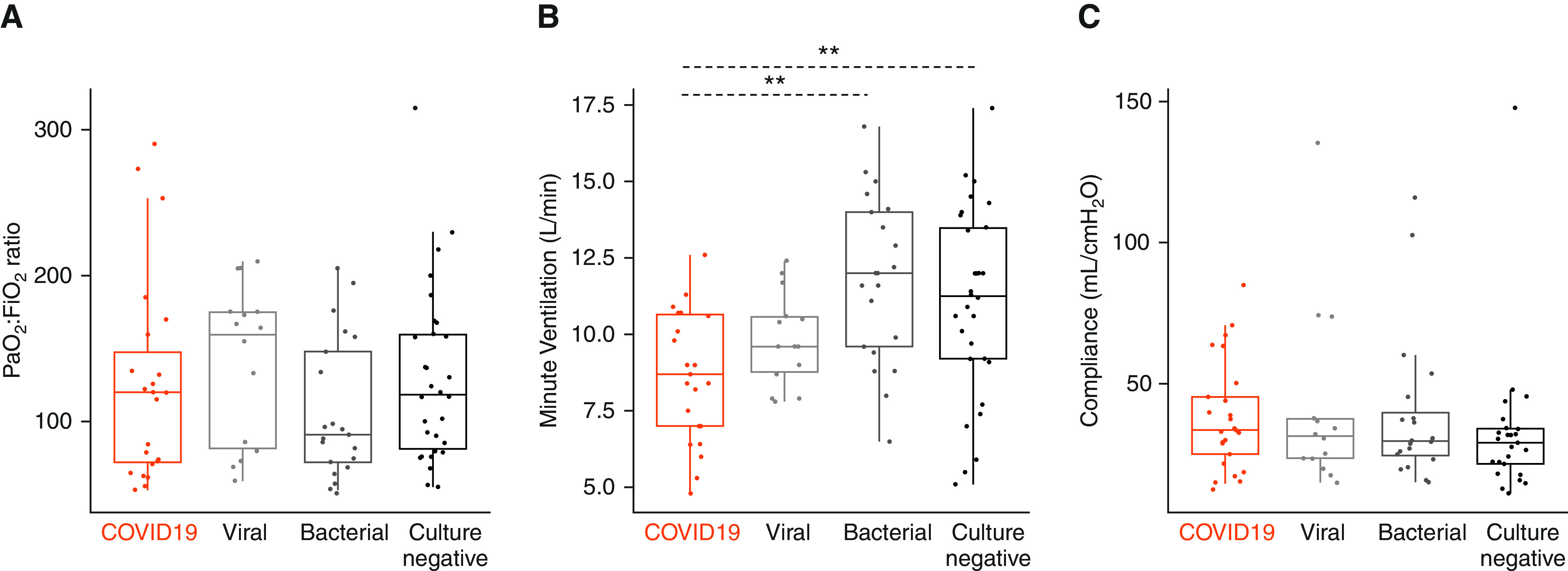
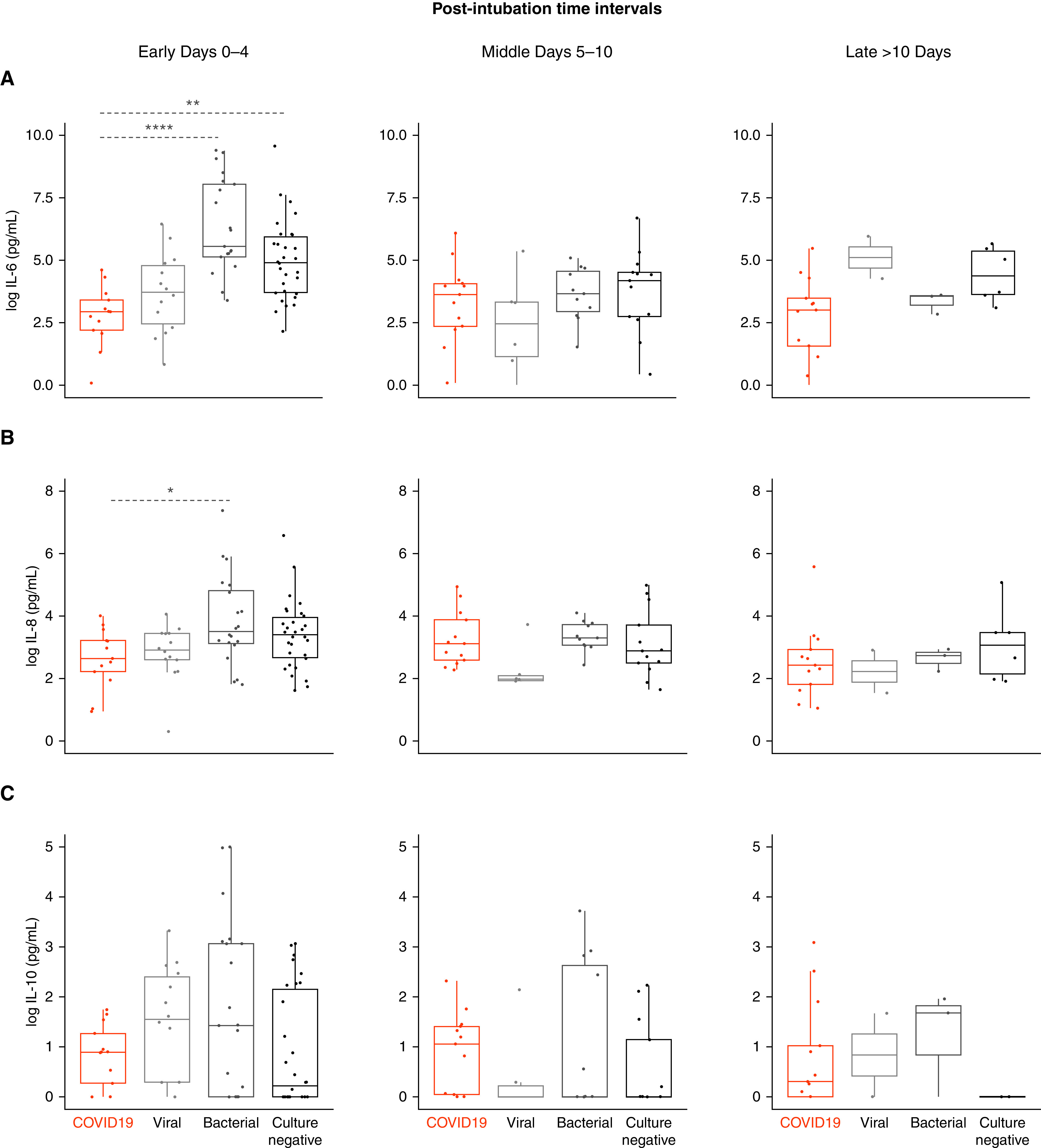
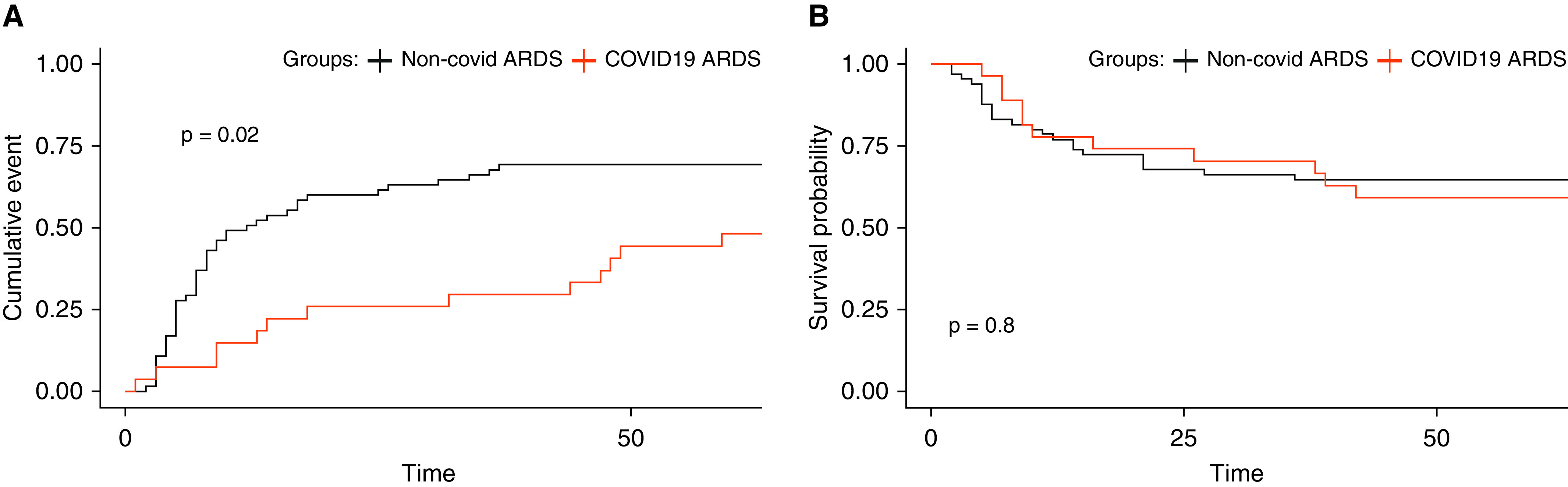
Rationale: There is an urgent need for improved understanding of the mechanisms and clinical characteristics of acute respiratory distress syndrome (ARDS) due to coronavirus disease (COVID-19).Objectives: To compare key demographic and physiologic parameters, biomarkers, and clinical outcomes of COVID-19 ARDS and ARDS secondary to direct lung injury from other etiologies of pneumonia.Methods: We enrolled 27 patients with COVID-19 ARDS in a prospective, observational cohort study and compared them with a historical, pre-COVID-19 cohort of patients with viral ARDS (n = 14), bacterial ARDS (n = 21), and ARDS due to culture-negative pneumonia (n = 30). We recorded clinical demographics; measured respiratory mechanical parameters; collected serial peripheral blood specimens for measurement of plasma interleukin (IL)-6, IL-8, and IL-10; and followed patients prospectively for patient-centered outcomes. We conducted between-group comparisons with nonparametric tests and analyzed time-to-event outcomes with Kaplan-Meier and Cox proportional hazards models.Results: Patients with COVID-19 ARDS had higher body mass index and were more likely to be Black, or residents of skilled nursing facilities, compared with those with non-COVID-19 ARDS (P < 0.05). Patients with COVID-19 had lower delivered minute ventilation compared with bacterial and culture-negative ARDS (post hoc P < 0.01) but not compared with viral ARDS. We found no differences in static compliance, hypoxemic indices, or carbon dioxide clearance between groups. Patients with COVID-19 had lower IL-6 levels compared with bacterial and culture-negative ARDS at early time points after intubation but no differences in IL-6 levels compared with viral ARDS. Patients with COVID-19 had longer duration of mechanical ventilation but similar 60-day mortality in both unadjusted and adjusted analyses.Conclusions: COVID-19 ARDS bears several similarities to viral ARDS but demonstrates lower minute ventilation and lower systemic levels of IL-6 compared with bacterial and culture-negative ARDS. COVID-19 ARDS was associated with longer dependence on mechanical ventilation compared with non-COVID-19 ARDS. Such detectable differences of COVID-19 do not merit deviation from evidence-based management of ARDS but suggest priorities for clinical research to better characterize and treat this new clinical entity.
Keywords: COVID-19; SARS-CoV-2; acute respiratory distress syndrome; pneumonia.
Figures
Comment in
-
Understanding COVID-19 Acute Respiratory Distress Syndrome.Ann Am Thorac Soc. 2022 Jan;19(1):150. doi: 10.1513/AnnalsATS.202104-486LE. Ann Am Thorac Soc. 2022. PMID: 34139146 Free PMC article. No abstract available.
-
Reply: Understanding COVID-19 Acute Respiratory Distress Syndrome: New Pathogen, Same Heterogeneous Syndrome.Ann Am Thorac Soc. 2022 Jan;19(1):151-160. doi: 10.1513/AnnalsATS.202106-650LE. Ann Am Thorac Soc. 2022. PMID: 34139147 Free PMC article. No abstract available.
Similar articles
-
A randomised, double-blind, placebo-controlled, pilot trial of intravenous plasma purified alpha-1 antitrypsin for SARS-CoV-2-induced Acute Respiratory Distress Syndrome: a structured summary of a study protocol for a randomised, controlled trial.Trials. 2021 Apr 19;22(1):288. doi: 10.1186/s13063-021-05254-0. Trials. 2021. PMID: 33874981 Free PMC article.
-
Flow controlled ventilation in Acute Respiratory Distress Syndrome associated with COVID-19: A structured summary of a study protocol for a randomised controlled trial.Trials. 2020 Sep 11;21(1):781. doi: 10.1186/s13063-020-04708-1. Trials. 2020. PMID: 32917259 Free PMC article.
-
Testing the efficacy and safety of BIO101, for the prevention of respiratory deterioration, in patients with COVID-19 pneumonia (COVA study): a structured summary of a study protocol for a randomised controlled trial.Trials. 2021 Jan 11;22(1):42. doi: 10.1186/s13063-020-04998-5. Trials. 2021. PMID: 33430924 Free PMC article.
-
Acute respiratory failure in COVID-19: is it "typical" ARDS?Crit Care. 2020 May 6;24(1):198. doi: 10.1186/s13054-020-02911-9. Crit Care. 2020. PMID: 32375845 Free PMC article. Review.
-
Understanding the pathophysiology of typical acute respiratory distress syndrome and severe COVID-19.Expert Rev Respir Med. 2022 Apr;16(4):437-446. doi: 10.1080/17476348.2022.2057300. Epub 2022 Mar 30. Expert Rev Respir Med. 2022. PMID: 35341424 Free PMC article. Review.
Cited by
-
Survival analysis of COVID-19 versus non-COVID-19 patients requiring intensive care for acute respiratory distress syndrome: An observational retrospective study.Can J Respir Ther. 2024 Aug 21;60:112-121. doi: 10.29390/001c.122402. eCollection 2024. Can J Respir Ther. 2024. PMID: 39268526 Free PMC article.
-
Inter-rater reliability and prognostic value of baseline Radiographic Assessment of Lung Edema (RALE) scores in observational cohort studies of inpatients with COVID-19.BMJ Open. 2023 Jan 12;13(1):e066626. doi: 10.1136/bmjopen-2022-066626. BMJ Open. 2023. PMID: 36635036 Free PMC article.
-
Time to Extubation in COVID-19 and Non-COVID-19 ARDS.Respir Care. 2023 Oct;68(10):1475-1476. doi: 10.4187/respcare.11411. Respir Care. 2023. PMID: 37722736 Free PMC article. No abstract available.
-
Mitochondrial N-formyl methionine peptides contribute to exaggerated neutrophil activation in patients with COVID-19.Virulence. 2023 Dec;14(1):2218077. doi: 10.1080/21505594.2023.2218077. Virulence. 2023. PMID: 37248708 Free PMC article.
-
Rehabilitative interventions in patients with persistent post COVID-19 symptoms-a review of recent advances and future perspectives.Eur Arch Psychiatry Clin Neurosci. 2024 Dec;274(8):1819-1828. doi: 10.1007/s00406-023-01631-9. Epub 2023 Jun 16. Eur Arch Psychiatry Clin Neurosci. 2024. PMID: 37326700 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
