

Cardiomyocyte Injury Following Acute Ischemic Stroke: Protocol for a Prospective Observational Cohort Study
- PMID: 33544087
- PMCID: PMC7895641
- DOI: 10.2196/24186
Cardiomyocyte Injury Following Acute Ischemic Stroke: Protocol for a Prospective Observational Cohort Study
Abstract
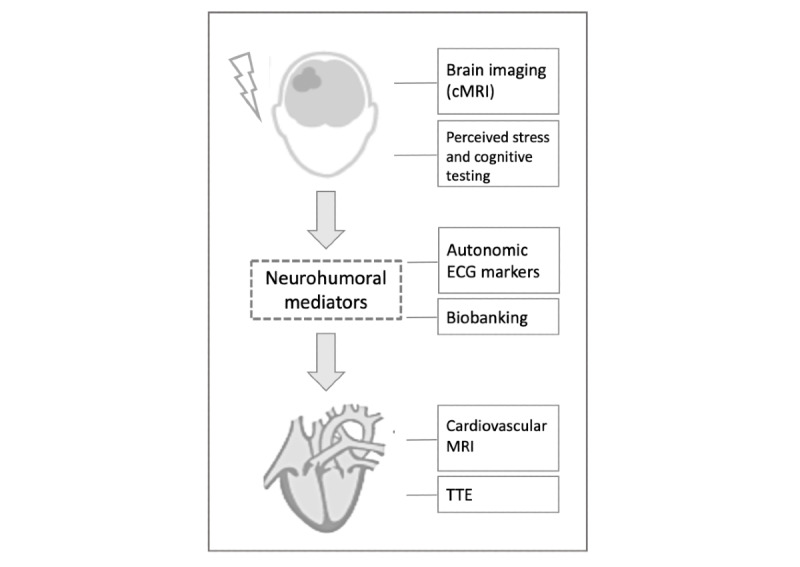
Background: Elevated cardiac troponin, which indicates cardiomyocyte injury, is common after acute ischemic stroke and is associated with poor functional outcome. Myocardial injury is part of a broad spectrum of cardiac complications that may occur after acute ischemic stroke. Previous studies have shown that in most patients, the underlying mechanism of stroke-associated myocardial injury may not be a concomitant acute coronary syndrome. Evidence from animal research and clinical and neuroimaging studies suggest that functional and structural alterations in the central autonomic network leading to stress-mediated neurocardiogenic injury may be a key underlying mechanism (ie, stroke-heart syndrome). However, the exact pathophysiological cascade remains unclear, and the diagnostic and therapeutic implications are unknown.
Objective: The aim of this CORONA-IS (Cardiomyocyte injury following Acute Ischemic Stroke) study is to quantify autonomic dysfunction and to decipher downstream cardiac mechanisms leading to myocardial injury after acute ischemic stroke.
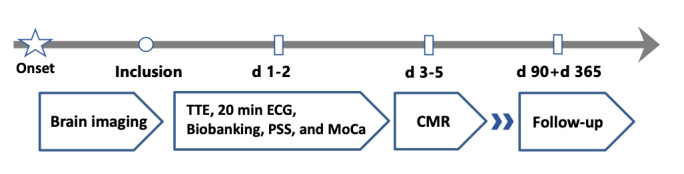
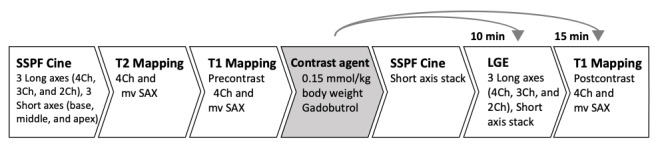
Methods: In this prospective, observational, single-center cohort study, 300 patients with acute ischemic stroke, confirmed via cerebral magnetic resonance imaging (MRI) and presenting within 48 hours of symptom onset, will be recruited during in-hospital stay. On the basis of high-sensitivity cardiac troponin levels and corresponding to the fourth universal definition of myocardial infarction, 3 groups are defined (ie, no myocardial injury [no cardiac troponin elevation], chronic myocardial injury [stable elevation], and acute myocardial injury [dynamic rise/fall pattern]). Each group will include approximately 100 patients. Study patients will receive routine diagnostic care. In addition, they will receive 3 Tesla cardiovascular MRI and transthoracic echocardiography within 5 days of symptom onset to provide myocardial tissue characterization and assess cardiac function, 20-min high-resolution electrocardiogram for analysis of cardiac autonomic function, and extensive biobanking. A follow-up for cardiovascular events will be conducted 3 and 12 months after inclusion.
Results: After a 4-month pilot phase, recruitment began in April 2019. We estimate a recruitment period of approximately 3 years to include 300 patients with a complete cardiovascular MRI protocol.
Conclusions: Stroke-associated myocardial injury is a common and relevant complication. Our study has the potential to provide a better mechanistic understanding of heart and brain interactions in the setting of acute stroke. Thus, it is essential to develop algorithms for recognizing patients at risk and to refine diagnostic and therapeutic procedures.
Trial registration: Clinicaltrials.gov NCT03892226; https://www.clinicaltrials.gov/ct2/show/NCT03892226.
International registered report identifier (irrid): DERR1-10.2196/24186.
Keywords: Takotsubo syndrome; autonomic nervous system; cardiac imaging techniques; ischemic stroke; magnetic resonance imaging; myocardial injury; myocardial ischemia; stroke-heart syndrome; troponin T.
©Helena Stengl, Ramanan Ganeshan, Simon Hellwig, Edyta Blaszczyk, Jochen B Fiebach, Christian H Nolte, Axel Bauer, Jeanette Schulz-Menger, Matthias Endres, Jan F Scheitz. Originally published in JMIR Research Protocols (http://www.researchprotocols.org), 05.02.2021.
Conflict of interest statement
Conflicts of Interest: ME received funding from Deutsche Forschungsgemeinschaft under Germany´s Excellence Strategy – EXC-2049 – 390688087, BMBF, DZNE, DZHK, EU, Corona Foundation, and Fondation Leducq. ME reports grants from Bayer and fees paid to the Charité from Bayer, Boehringer Ingelheim, BMS, Daiichi Sankyo, Amgen, GSK, Sanofi, Covidien, Novartis, Pfizer, all outside the submitted work.
Figures
References
-
- Wrigley P, Khoury J, Eckerle B, Alwell K, Moomaw CJ, Woo D, Flaherty ML, De Los Rios la Rosa F, Mackey J, Adeoye O, Martini S, Ferioli S, Kissela BM, Kleindorfer DO. Prevalence of Positive Troponin and Echocardiogram Findings and Association With Mortality in Acute Ischemic Stroke. Stroke. 2017 May;48(5):1226–32. doi: 10.1161/STROKEAHA.116.014561. http://europepmc.org/abstract/MED/28381647 - DOI - PMC - PubMed
-
- Scheitz JF, Mochmann H, Erdur H, Tütüncü S, Haeusler KG, Grittner U, Laufs U, Endres M, Nolte CH. Prognostic relevance of cardiac troponin T levels and their dynamic changes measured with a high-sensitivity assay in acute ischaemic stroke: analyses from the TRELAS cohort. Int J Cardiol. 2014 Dec 20;177(3):886–93. doi: 10.1016/j.ijcard.2014.10.036. - DOI - PubMed
-
- Faiz KW, Thommessen B, Einvik G, Brekke PH, Omland T, Ronning OM. Determinants of high sensitivity cardiac troponin T elevation in acute ischemic stroke. BMC Neurol. 2014 May 03;14:96. doi: 10.1186/1471-2377-14-96. https://bmcneurol.biomedcentral.com/articles/10.1186/1471-2377-14-96 - DOI - PMC - PubMed
-
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD, Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction Fourth Universal Definition of Myocardial Infarction (2018) J Am Coll Cardiol. 2018 Oct 30;72(18):2231–2264. doi: 10.1016/j.jacc.2018.08.1038. https://linkinghub.elsevier.com/retrieve/pii/S0735-1097(18)36941-9 - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
