

Oncological outcome after local treatment for early stage rectal cancer
- PMID: 33544250
- PMCID: PMC8741713
- DOI: 10.1007/s00464-021-08308-1
Oncological outcome after local treatment for early stage rectal cancer
Abstract
Background: Treatment of early rectal cancer is evolving towards organ-preserving therapy which includes endoscopic resection and transanal approaches. We aimed to explore the role of local treatments such as endoscopic polypectomy (Endoscopic Mucosal Resection (EMR) or Endoscopic submucosal dissection (ESD)) and transanal endoscopic microsurgery/ transanal minimal invasive surgery (TEM/TAMIS) in patients who had early rectal cancer. We considered these outcomes alongside conventional major surgery using total mesorectal excision (TME) for early stage disease.
Methods: All patients identified at MDT with early stage rectal cancer at our institution between 2010 and 2019 were included. Long-term outcomes in terms of local recurrence, survival and procedure-specific morbidity were analysed.
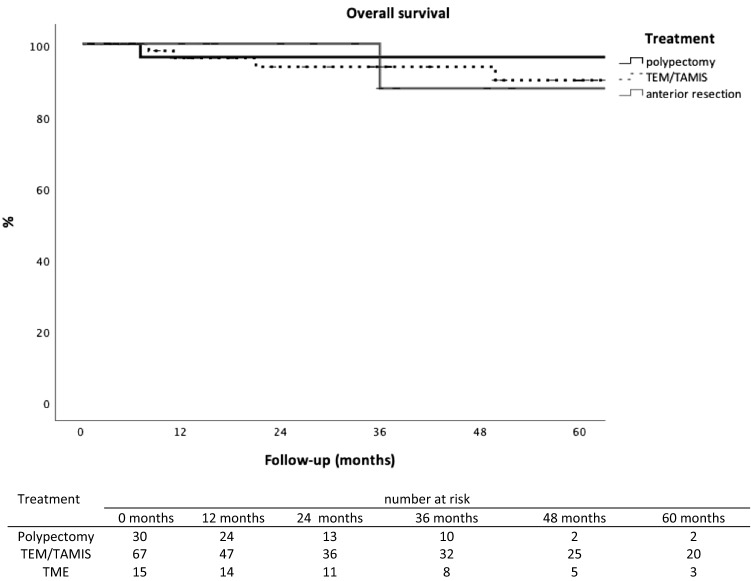
Results: In total, 536 patients with rectal cancer were identified, of which 112 were included based on their pre-operative identification at the MDT on the basis that they had node-negative early rectal cancer. Among these, 30 patients (27%) had the lesion excised by flexible endoscopic polypectomy techniques (EMR/ESD), 67 (60%) underwent TEM/TAMIS and 15 (13%) had major surgery. There were no differences in patient demographics between the three groups except for TEM/TAMIS patients being more likely to be referred from another hospital (p < 0.001) and they were less active (WHO performance status p = 0.04). There were no significant differences in overall survival rates and cancer-specific survival between the three treatment groups. The 5-year overall survival rate for endoscopic polypectomy, TEM/TAMIS or major resection was 96% versus 90% and 88%, respectively (p = 0.89). The 5- year cancer-specific survival rate was 96%, versus 96% and 100%, respectively (p = 0.74).
Conclusion: Endoscopic polypectomy by EMR/ESD is an appropriate local treatment for early stage rectal cancer in selected patients. It is possible to achieve good oncological outcomes with a polypectomy similar to TEM/TAMIS and major surgery; however, a multidisciplinary approach is necessary enabling close surveillance and the use of adjuvant radiotherapy.
Keywords: Early rectal cancer; Local treatment; Polypectomy (EMR/ESD); TAMIS; TEM.
© 2021. The Author(s).
Conflict of interest statement
James East has served on clinical advisory board for Lumendi, Boston Scientific and Paion; Clinical advisory board and ownership, Satisfai Health; Speaker fees, Falk. Caroline Witjes, Abhilashaben Patel, Aniruddh Shenoy, Stephen Boyce, James East and Christopher Cunningham have no conflicts of interest or financial ties to disclose.
Figures


References
-
- Battersby NJ, Juul T, Christensen P, Janjua AZ, Branagan G, Emmertsen KJ, Norton C, Hughes R, Laurberg S, Moran BJ, United Kingdom Low Anterior Resection Syndrome Study Group (2016) Predicting the risk of bowel-related quality-of-life impairment after restorative resection for rectal cancer: a multicenter cross-sectional study. Dis Colon Rectum 59(4):270–280 - PubMed
-
- Martens MH, Maas M, Heijnen LA, Lambregts DMJ, Leijtens JWA, Stassen LPS, Breukink SO, Hoff C, Belgers EJ, Melenhorst J, Jansen R, Buijsen J, Hoofwijk TGM, Beets-Tan GH, Beets GL (2016) Long-term outcome of an organ preservation program after neoajuvant treatment for rectal cancer. J Natl Cancer Inst 108(12) - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
