

Osimertinib Versus Comparator EGFR TKI as First-Line Treatment for EGFR-Mutated Advanced NSCLC: FLAURA China, A Randomized Study
- PMID: 33544337
- PMCID: PMC7935816
- DOI: 10.1007/s11523-021-00794-6
Osimertinib Versus Comparator EGFR TKI as First-Line Treatment for EGFR-Mutated Advanced NSCLC: FLAURA China, A Randomized Study
Abstract
Background: In the global FLAURA study, first-line osimertinib, a third-generation irreversible tyrosine kinase inhibitor (TKI) of epidermal growth factor receptor (EGFR), significantly improved progression-free survival (PFS) and overall survival (OS) versus comparator EGFR TKIs in patients with EGFR mutation-positive (EGFRm) advanced non-small-cell lung cancer (NSCLC).
Objective: The FLAURA China study assessed first-line osimertinib in Chinese patients with EGFRm advanced NSCLC (NCT02296125).
Methods: FLAURA China was a double-blind, randomized, phase III study. Adults from mainland China with previously untreated EGFRm (Exon 19 deletion or L858R) advanced NSCLC were enrolled in the global study or a China-only study under the same protocol; 136 patients were randomized to osimertinib (80 mg once daily [od]; n = 71) or comparator EGFR TKI (gefitinib or erlotinib; all sites selected gefitinib 250 mg od; n = 65). Patients were randomized and allocated to treatment groups by a central computer system. Treatment continued until disease progression, unacceptable toxicity, or withdrawal of consent. The primary endpoint was investigator-assessed PFS; OS was a secondary endpoint.
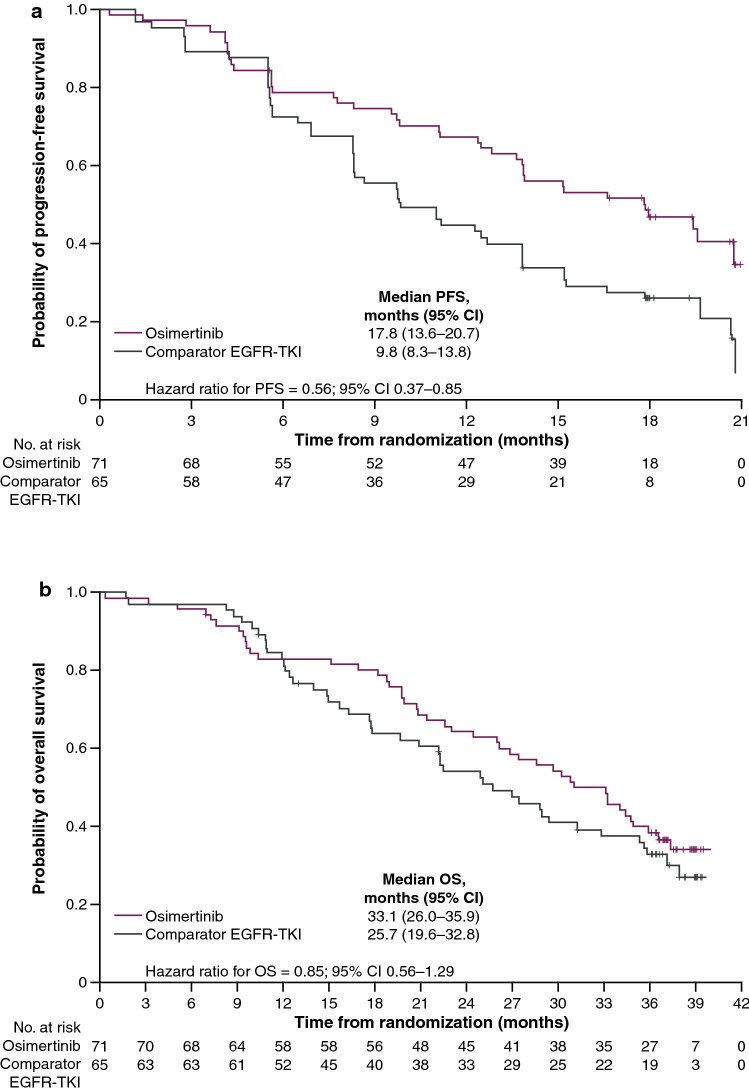
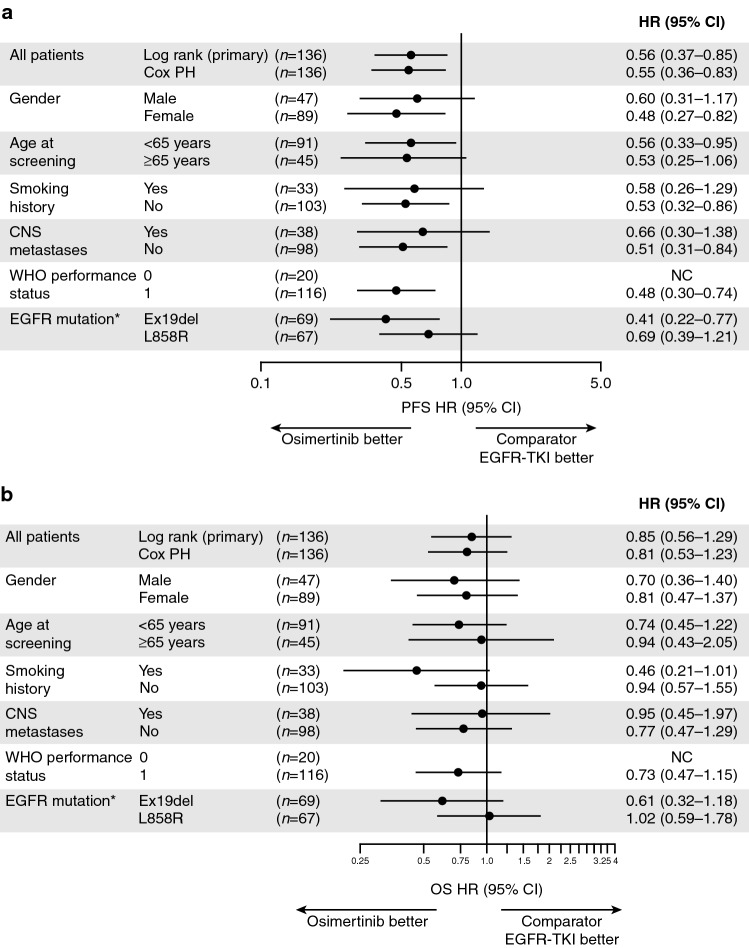
Results: All 136 randomized patients were analyzed. Osimertinib extended median PFS by 8.0 months versus comparator EGFR TKI (17.8 vs. 9.8 months; hazard ratio [HR] 0.56; 95% confidence interval [CI] 0.37-0.85). Median OS was 33.1 months in the osimertinib group versus 25.7 months in the comparator group (HR 0.85; 95% CI 0.56-1.29). At 3 years, 20% of patients on osimertinib and 8% on the comparator remained on randomized treatment. Grade 3 or higher adverse events (AEs) were reported in 54 and 28% of patients in the osimertinib and comparator groups, respectively, driven by increased local reporting of laboratory- and disease-related AEs. No new safety signals were identified.
Conclusions: First-line osimertinib treatment resulted in a clinically meaningful PFS and OS benefit versus comparator EGFR TKI in Chinese patients with EGFRm advanced NSCLC. Safety data were consistent with the known safety profile of osimertinib.
Clinical trial registration: ClinicalTrials.gov NCT02296125, registered 20 November 2014.
Conflict of interest statement
YC, WL, HZ, and CL have no conflicts of interest that are directly relevant to the content of this article. YH has received personal fees from AstraZeneca, Eli Lilly, Pfizer, and Roche for speaker bureau/expert testimony. QZ has received personal honoraria from AstraZeneca and Roche. BW has received personal fees from AstraZeneca, Boehringer Ingelheim, and Roche for advisory/consultancy and speaker bureau/expert testimony and from Eli Lilly for speaker bureau/expert testimony. AW, MS, and XH are employees and shareholders/stockholders of and hold stock options for AstraZeneca. MF received personal fees from AstraZeneca during the conduct of the study and is an employee of AstraZeneca. JW is an employee of AstraZeneca. SSR has received grants and personal fees from Amgen, BMS, Merck, Tesaro, and Takeda; grants from Advaxis and Genmab; grants, personal fees, and non-financial support from AstraZeneca; and personal fees from Genentech and Glaxo Smith Kline, outside the submitted work.
Figures
References
-
- Liang H, Song X, Zhang Y, Zhang S, Li F, Fang J, et al. Real-world data on EGFR/ALK gene status and first-line targeted therapy rate in newly diagnosed advanced non-small cell lung cancer patients in Northern China: a prospective observational study. Thorac Cancer. 2019;10(7):1521–1532. doi: 10.1111/1759-7714.13090. - DOI - PMC - PubMed
-
- Wu YL, Planchard D, Lu S, Sun H, Yamamoto N, Kim DW, et al. Pan-Asian adapted Clinical Practice Guidelines for the management of patients with metastatic non-small-cell lung cancer: a CSCO-ESMO initiative endorsed by JSMO, KSMO, MOS. SSO and TOS. Ann Oncol. 2019;30(2):171–210. doi: 10.1093/annonc/mdy554. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
