

Airborne aerosol olfactory deposition contributes to anosmia in COVID-19
- PMID: 33544701
- PMCID: PMC7864464
- DOI: 10.1371/journal.pone.0244127
Airborne aerosol olfactory deposition contributes to anosmia in COVID-19
Abstract
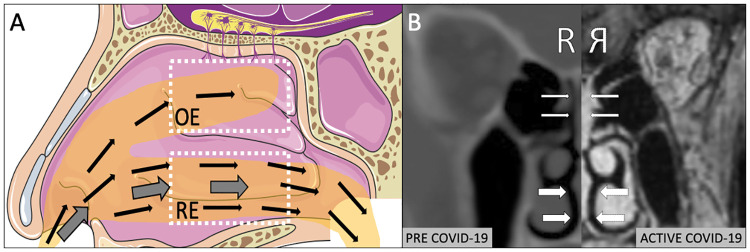
Introduction: Olfactory dysfunction (OD) affects a majority of COVID-19 patients, is atypical in duration and recovery, and is associated with focal opacification and inflammation of the olfactory epithelium. Given recent increased emphasis on airborne transmission of SARS-CoV-2, the purpose of the present study was to experimentally characterize aerosol dispersion within olfactory epithelium (OE) and respiratory epithelium (RE) in human subjects, to determine if small (sub 5μm) airborne aerosols selectively deposit in the OE.
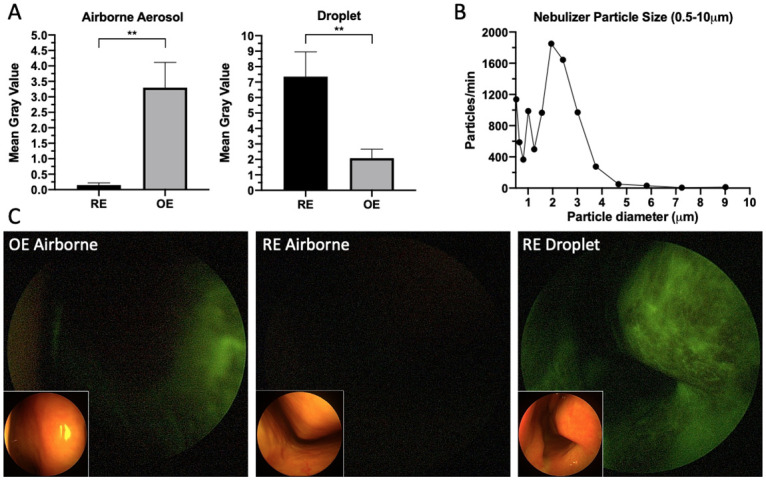
Methods: Healthy adult volunteers inhaled fluorescein-labeled nebulized 0.5-5μm airborne aerosol or atomized larger aerosolized droplets (30-100μm). Particulate deposition in the OE and RE was assessed by blue-light filter modified rigid endoscopic evaluation with subsequent image randomization, processing and quantification by a blinded reviewer.
Results: 0.5-5μm airborne aerosol deposition, as assessed by fluorescence gray value, was significantly higher in the OE than the RE bilaterally, with minimal to no deposition observed in the RE (maximum fluorescence: OE 19.5(IQR 22.5), RE 1(IQR 3.2), p<0.001; average fluorescence: OE 2.3(IQR 4.5), RE 0.1(IQR 0.2), p<0.01). Conversely, larger 30-100μm aerosolized droplet deposition was significantly greater in the RE than the OE (maximum fluorescence: OE 13(IQR 14.3), RE 38(IQR 45.5), p<0.01; average fluorescence: OE 1.9(IQR 2.1), RE 5.9(IQR 5.9), p<0.01).
Conclusions: Our data experimentally confirm that despite bypassing the majority of the upper airway, small-sized (0.5-5μm) airborne aerosols differentially deposit in significant concentrations within the olfactory epithelium. This provides a compelling aerodynamic mechanism to explain atypical OD in COVID-19.
Conflict of interest statement
The authors do not have competing interests that could bias this work.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
