

Resting state EEG biomarkers of cognitive decline associated with Alzheimer's disease and mild cognitive impairment
- PMID: 33544703
- PMCID: PMC7864432
- DOI: 10.1371/journal.pone.0244180
Resting state EEG biomarkers of cognitive decline associated with Alzheimer's disease and mild cognitive impairment
Abstract
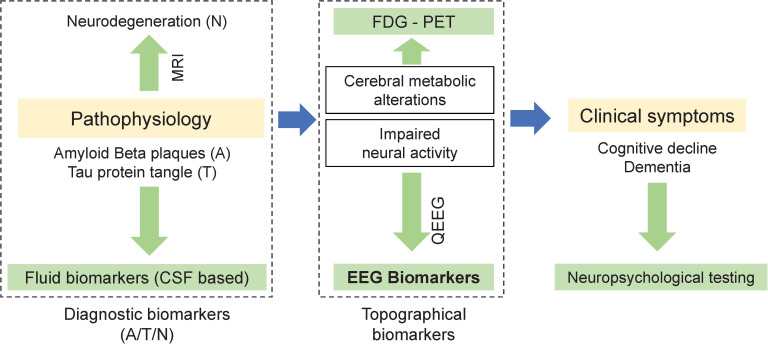
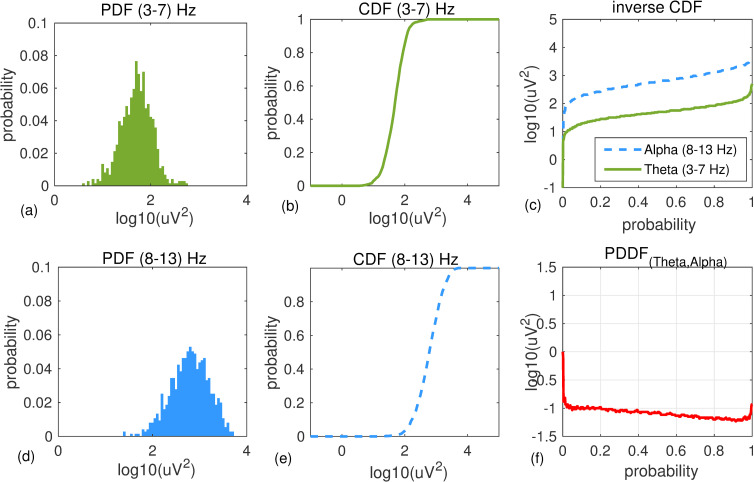
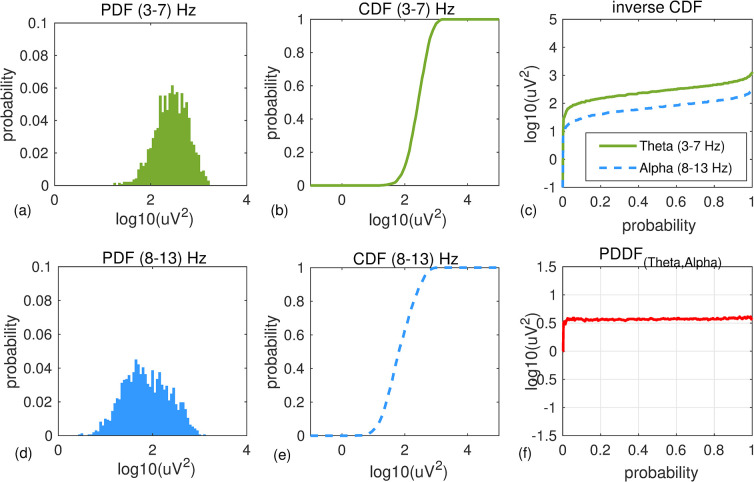
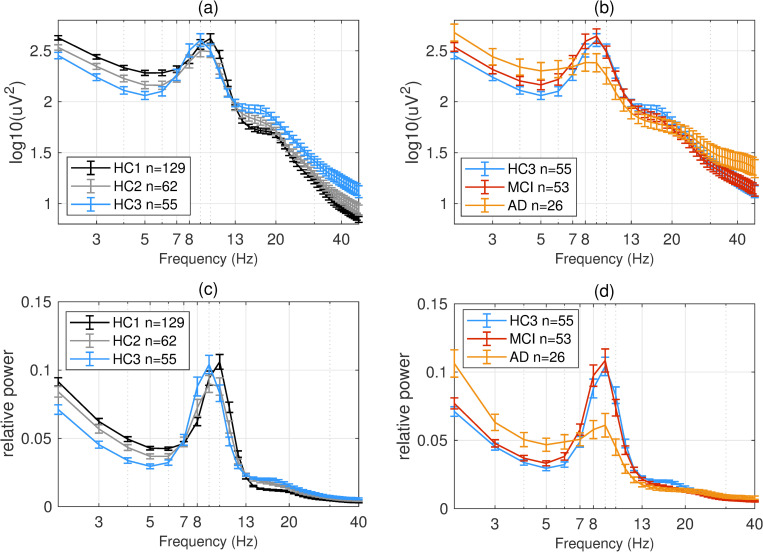
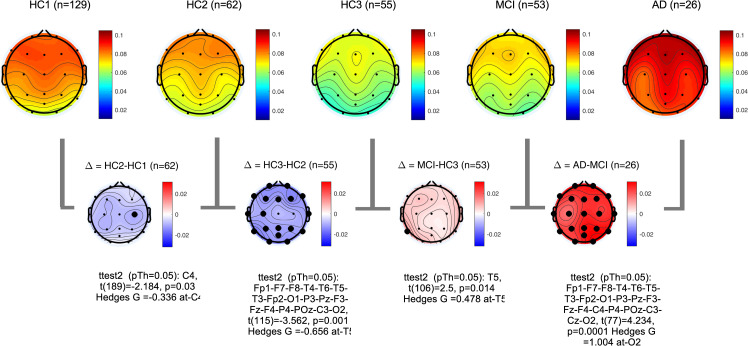
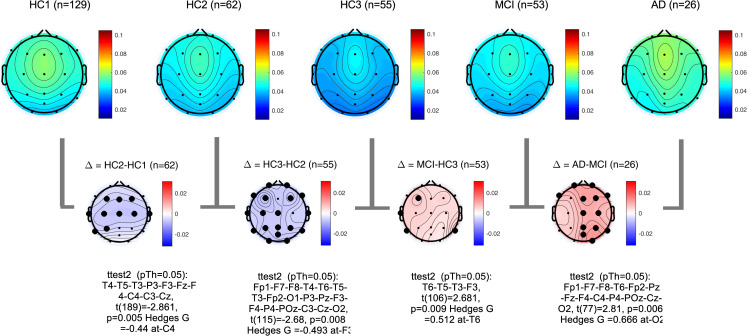
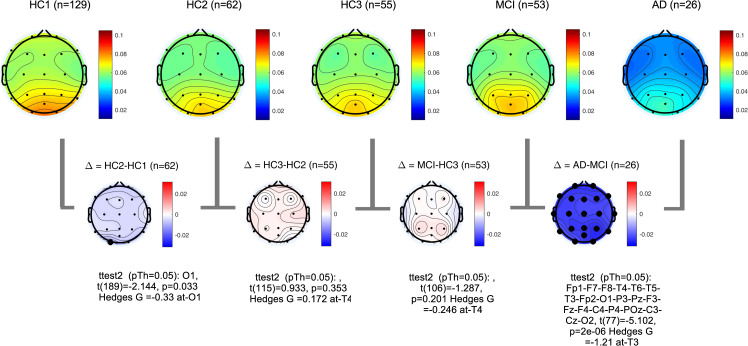
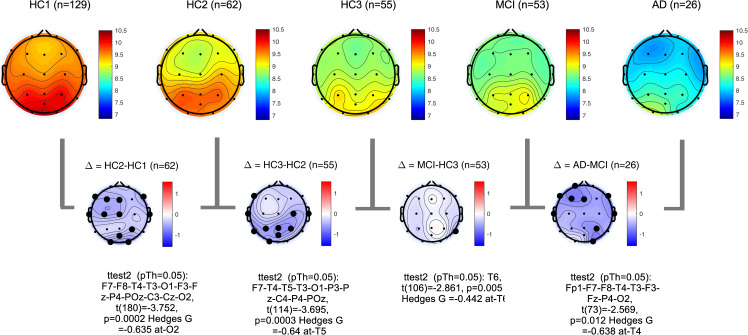
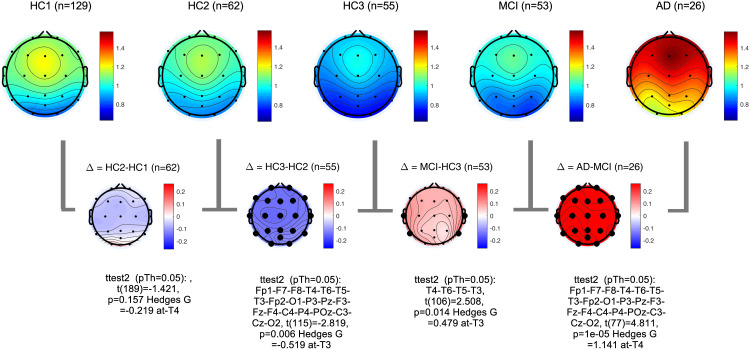
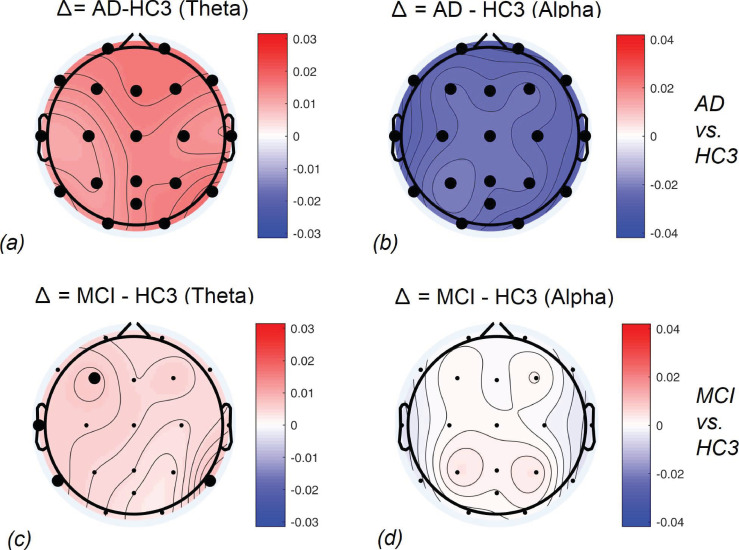
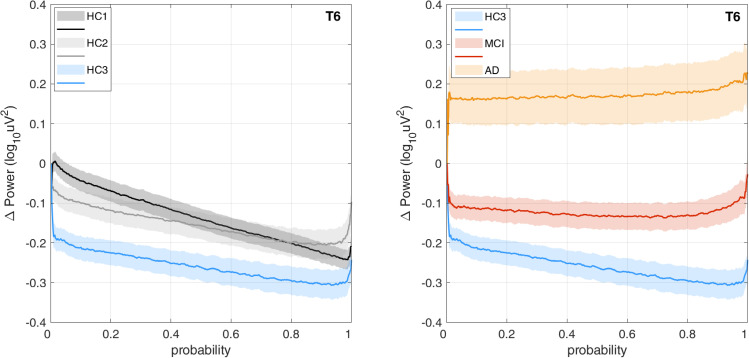
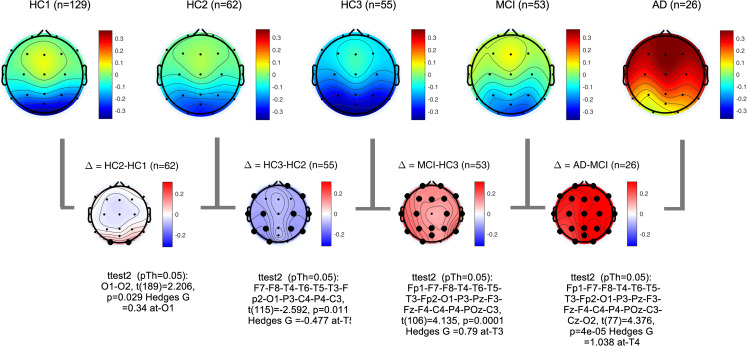
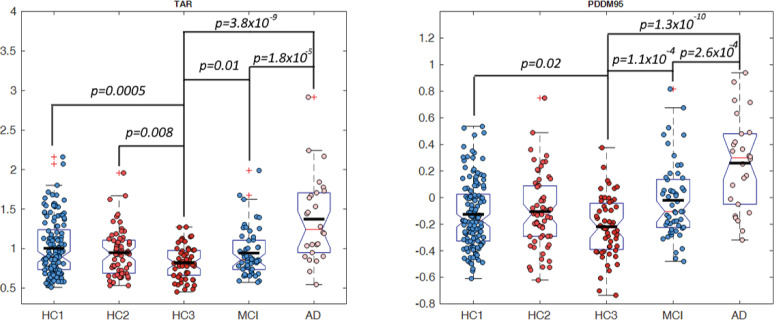
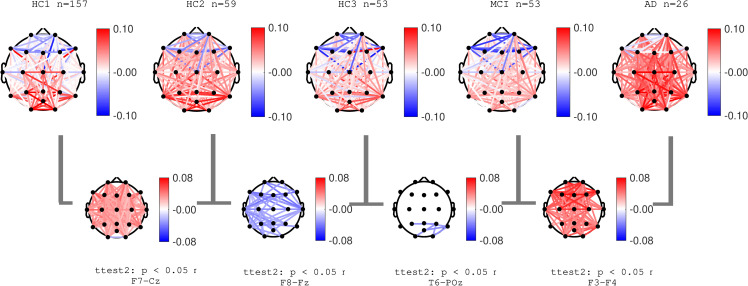
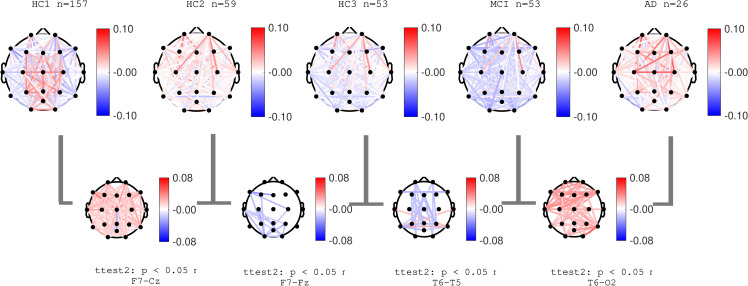
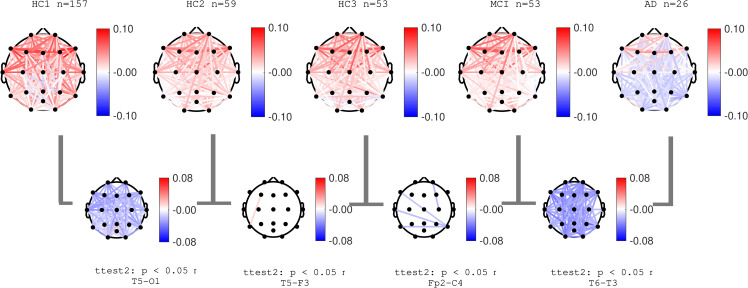
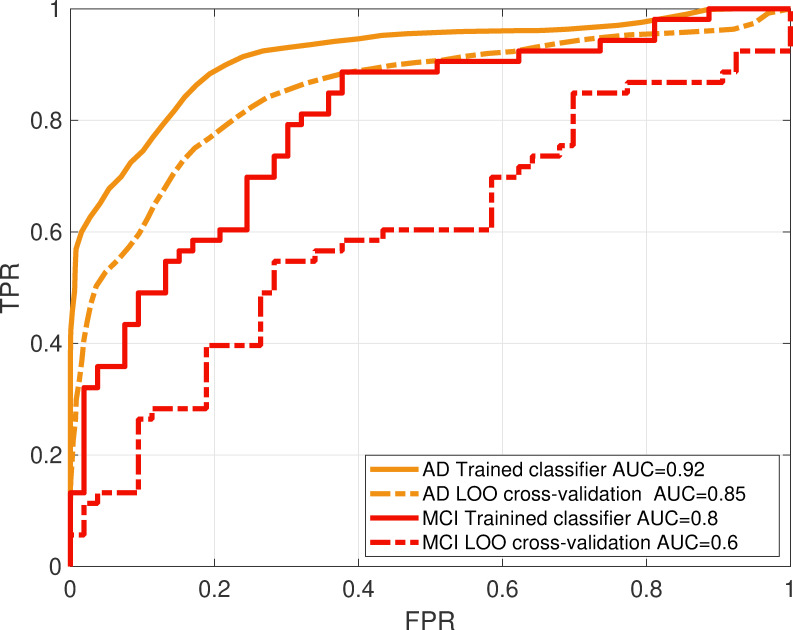
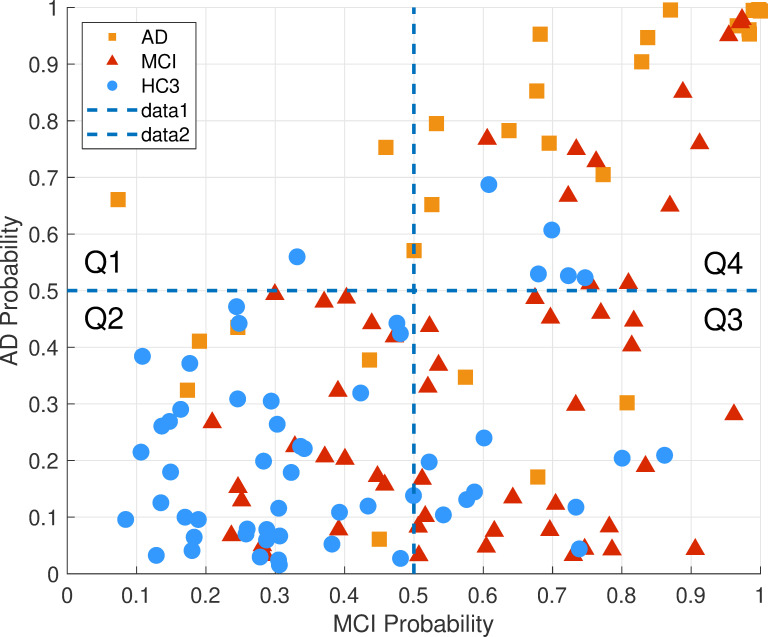
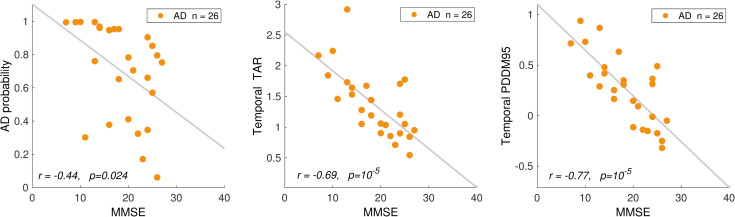
In this paper, we explore the utility of resting-state EEG measures as potential biomarkers for the detection and assessment of cognitive decline in mild cognitive impairment (MCI) and Alzheimer's disease (AD). Neurophysiological biomarkers of AD derived from EEG and FDG-PET, once characterized and validated, would expand the set of existing diagnostic molecular biomarkers of AD pathology with associated biomarkers of disease progression and neural dysfunction. Since symptoms of AD often begin to appear later in life, successful identification of EEG-based biomarkers must account for age-related neurophysiological changes that occur even in healthy individuals. To this end, we collected EEG data from individuals with AD (n = 26), MCI (n = 53), and cognitively normal healthy controls stratified by age into three groups: 18-40 (n = 129), 40-60 (n = 62) and 60-90 (= 55) years old. For each participant, we computed power spectral density at each channel and spectral coherence between pairs of channels. Compared to age matched controls, in the AD group, we found increases in both spectral power and coherence at the slower frequencies (Delta, Theta). A smaller but significant increase in power of slow frequencies was observed for the MCI group, localized to temporal areas. These effects on slow frequency spectral power opposed that of normal aging observed by a decrease in the power of slow frequencies in our control groups. The AD group showed a significant decrease in the spectral power and coherence in the Alpha band consistent with the same effect in normal aging. However, the MCI group did not show any significant change in the Alpha band. Overall, Theta to Alpha ratio (TAR) provided the largest and most significant differences between the AD group and controls. However, differences in the MCI group remained small and localized. We proposed a novel method to quantify these small differences between Theta and Alpha bands' power using empirically derived distributions of spectral power across the time domain as opposed to averaging power across time. We defined Power Distribution Distance Measure (PDDM) as a distance measure between probability distribution functions (pdf) of Theta and Alpha power. Compared to average TAR, using PDDF enhanced the statistical significance, the effect size, and the spatial distribution of significant effects in the MCI group. We designed classifiers for differentiating individual MCI and AD participants from age-matched controls. The classification performance measured by the area under ROC curve after cross-validation were AUC = 0.85 and AUC = 0.6, for AD and MCI classifiers, respectively. Posterior probability of AD, TAR, and the proposed PDDM measure were all significantly correlated with MMSE score and neuropsychological tests in the AD group.
Conflict of interest statement
AM, MSK, MM, GR, CR and CB are employees of Advanced Brain Monitoring. Chris Berka is co-founder and shareholder of Advanced Brain Monitoring. Advanced Brain Monitoring is a commercial medical device manufacturer specializing in the acquisition and analysis of EEG during wake and sleep. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Jack C. R. et al., “Introduction to the recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease,” Alzheimers Dement. J. Alzheimers Assoc., vol. 7, no. 3, pp. 257–262, May 2011, 10.1016/j.jalz.2011.03.004 - DOI - PMC - PubMed
-
- Sperling R. A. et al., “Toward defining the preclinical stages of Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease,” Alzheimers Dement. J. Alzheimers Assoc., vol. 7, no. 3, pp. 280–292, May 2011, 10.1016/j.jalz.2011.03.003 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
