

A Phase 2 Study of Capmatinib in Patients With MET-Altered Lung Cancer Previously Treated With a MET Inhibitor
- PMID: 33545388
- PMCID: PMC8922989
- DOI: 10.1016/j.jtho.2021.01.1605
A Phase 2 Study of Capmatinib in Patients With MET-Altered Lung Cancer Previously Treated With a MET Inhibitor
Abstract
Introduction: Capmatinib is approved for MET exon 14-altered NSCLC on the basis of activity in targeted therapy-naive patients. We conducted a phase 2 study to assess the efficacy of capmatinib in patients previously treated with a MET inhibitor.
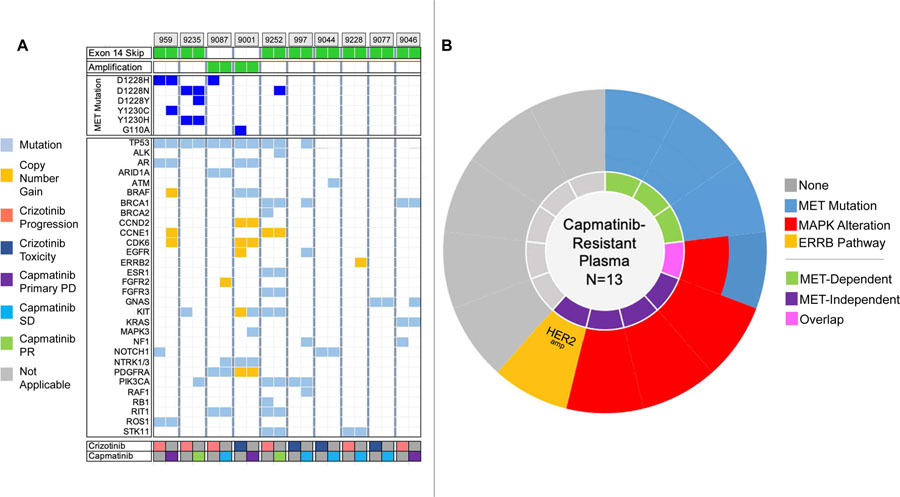
Methods: Patients with advanced NSCLC harboring MET amplification or MET exon 14 skipping alterations received capmatinib 400 mg twice daily. The primary end point was the objective response rate. Secondary end points included progression-free survival, disease control rate (DCR), intracranial response rate, and overall survival. Circulating tumor DNA was analyzed to identify capmatinib resistance mechanisms.
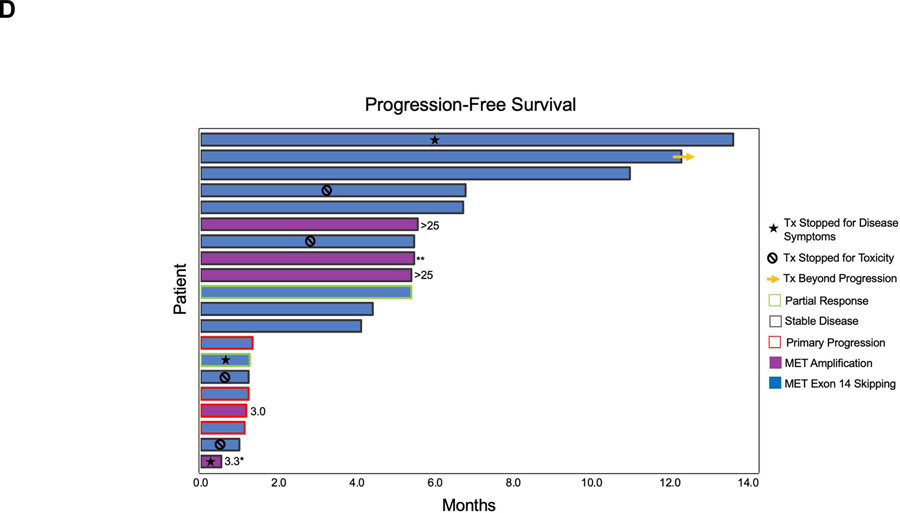
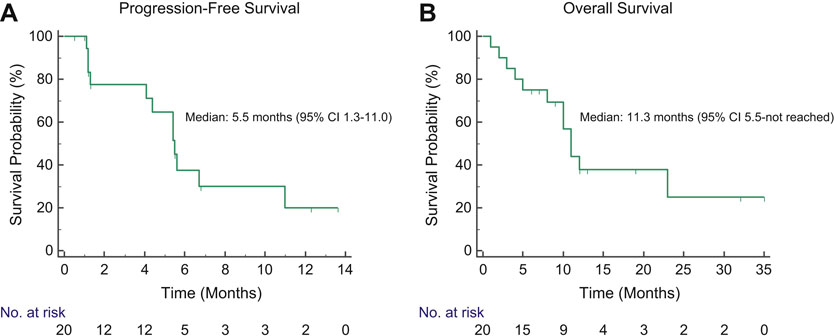
Results: A total of 20 patients were enrolled between May 2016 and November 2019, including 15 patients with MET skipping alterations and five patients with MET amplification. All patients had received crizotinib; three had also received other MET-directed therapies. The median interval between crizotinib and capmatinib was 22 days (range: 4-374). Two patients (10%) achieved an objective response to capmatinib and 14 had stable disease, yielding a DCR of 80%. Among five patients who discontinued crizotinib for intolerance, the DCR was 83%, including two patients with the best tumor shrinkage of -25% and -28%. Intracranial DCR among four patients with measurable brain metastases was 100%, with no observed intracranial objective responses. Overall, the median progression-free survival and overall survival were 5.5 (95% confidence interval: 1.3-11.0) and 11.3 (95% confidence interval: 5.5-not reached) months, respectively. MET D1228 and Y1230 mutations and MAPK alterations were recurrently detected in postcrizotinib, precapmatinib plasma. New and persistent MET mutations and MAPK pathway alterations were detected in plasma at progression on capmatinib.
Conclusions: Capmatinib has modest activity in crizotinib-pretreated MET-altered NSCLC, potentially owing to overlapping resistance mechanisms.
Keywords: Capmatinib; Lung cancer; MET amplification; MET skipping.
Copyright © 2021 International Association for the Study of Lung Cancer. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
Sequencing of MET Inhibitors in Lung Cancer: Have We Met the Target?J Thorac Oncol. 2021 May;16(5):709-711. doi: 10.1016/j.jtho.2021.02.017. J Thorac Oncol. 2021. PMID: 33896567 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
