

Evaluation of Antibody Response in Symptomatic and Asymptomatic COVID-19 Patients and Diagnostic Assessment of New IgM/IgG ELISA Kits
- PMID: 33546341
- PMCID: PMC7913500
- DOI: 10.3390/pathogens10020161
Evaluation of Antibody Response in Symptomatic and Asymptomatic COVID-19 Patients and Diagnostic Assessment of New IgM/IgG ELISA Kits
Abstract
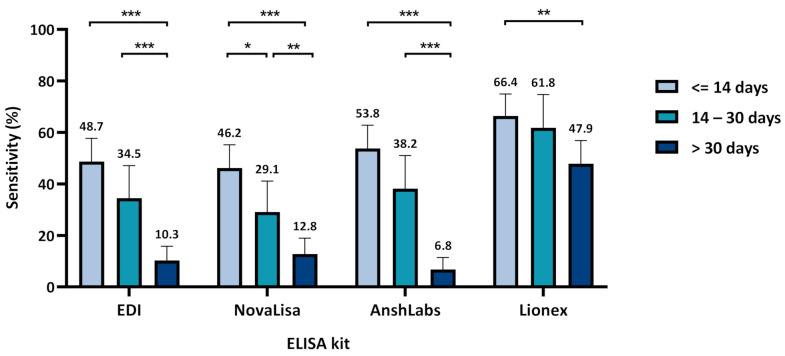
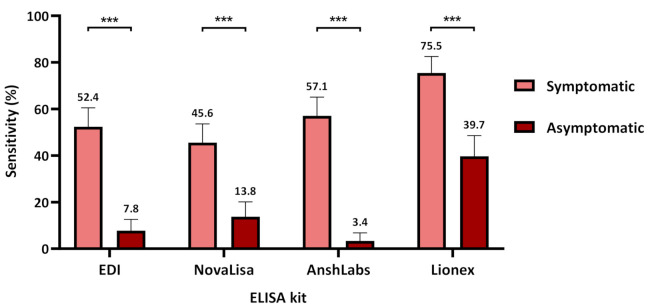
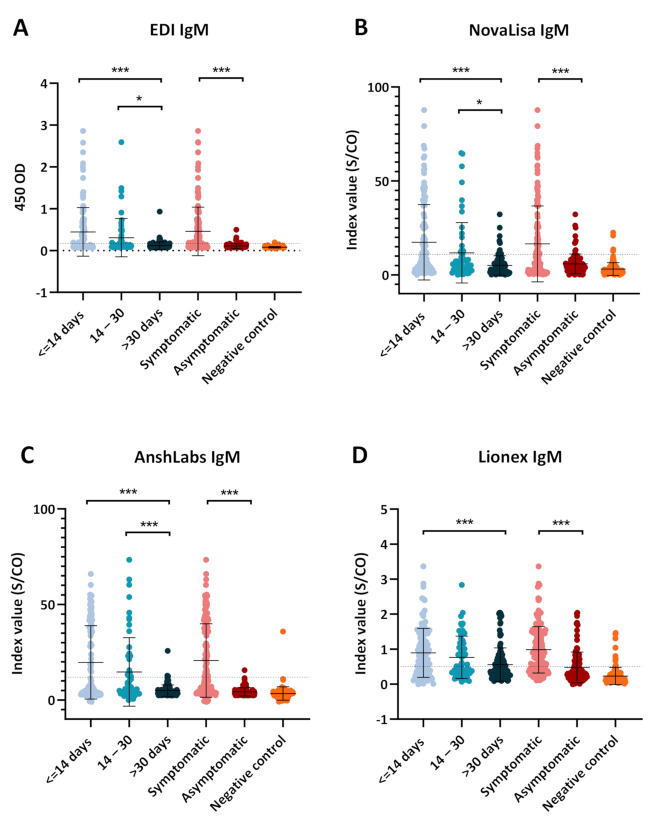
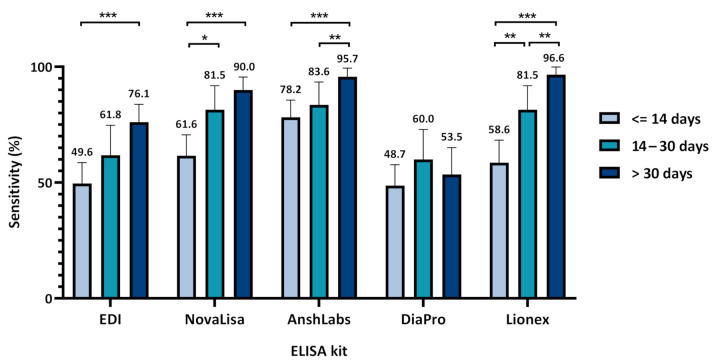
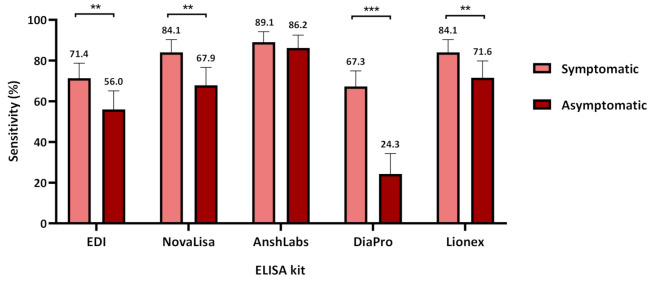
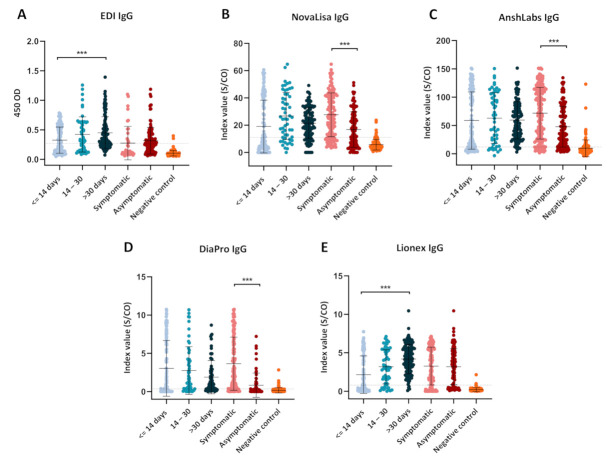
This study aims to study the immune response and evaluate the performances of four new IgM and five IgG enzyme-linked immunosorbent assay (ELISA) kits for detecting anti-severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) antibodies against different antigens in symptomatic and asymptomatic coronavirus disease 2019 (COVID-19) patients. A total of 291 samples collected from symptomatic and asymptomatic RT-PCR-confirmed patients were used to evaluate the ELISA kits' performance (EDI, AnshLabs, DiaPro, NovaLisa, and Lionex). The sensitivity was measured at three different time-intervals post symptoms onset or positive SARS-CoV-2 RT-PCR test (≤14, 14-30, >30 days). The specificity was investigated using 119 pre-pandemic serum samples. The sensitivity of all IgM kits gradually decreased with time, ranging from 48.7% (EDI)-66.4% (Lionex) at ≤14 days, 29.1% (NovaLisa)-61.8% (Lionex) at 14-30 days, and 6.0% (AnshLabs)-47.9% (Lionex) at >30 days. The sensitivity of IgG kits increased with time, peaking in the latest interval (>30 days) at 96.6% (Lionex). Specificity of IgM ranged from 88.2% (Lionex)-99.2% (EDI), while IgG ranged from 75.6% (DiaPro)-98.3% (Lionex). Among all RT-PCR-positive patients, 23 samples (7.9%) were seronegative by all IgG kits, of which only seven samples (30.4%) had detectable IgM antibodies. IgM assays have variable and low sensitivity, thus considered a poor marker for COVID-19 diagnosis. IgG assays can miss at least 8% of RT-PCR-positive cases.
Keywords: COVID-19; ELISA; IgG; IgM; SARS-CoV-2; asymptomatic; sensitivity; serology; specificity; symptomatic.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Dobaño C., Vidal M., Santano R., Jiménez A., Chi J., Barrios D., Ruiz-Olalla G., Melero N.R., Carolis C., Parras D., et al. Highly sensitive and specific multiplex antibody assays to quantify immunoglobulins M, A and G against SARS-CoV-2 antigens. bioRxiv. 2020 doi: 10.1128/JCM.01731-20. - DOI - PMC - PubMed
-
- Adams E.R., Anand R., Andersson M.I., Auckland K., Baillie J.K., Barnes E., Bell J., Berry T., Bibi S., Carroll M., et al. Evaluation of antibody testing for SARS-Cov-2 using ELISA and lateral flow immunoassays. medRxiv. 2020 doi: 10.1101/2020.04.15.20066407. - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
