

Anti-HEV IgG Avidity Testing: Utility for Diagnosing Acute and Resolved Genotype 3 Infections
- PMID: 33546482
- PMCID: PMC7913725
- DOI: 10.3390/v13020236
Anti-HEV IgG Avidity Testing: Utility for Diagnosing Acute and Resolved Genotype 3 Infections
Abstract
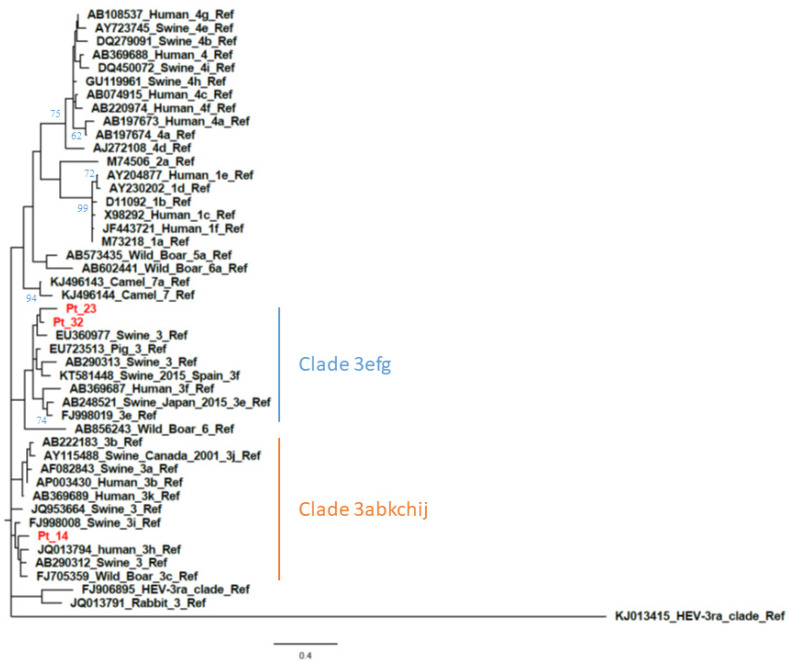
European Association of the Study of the Liver (EASL) guidelines specify HEV RNA, as well as anti-HEV IgG and IgM as positive markers for acute HEV infection. HEV RNA assay sensitivity limitations may lead to false negative test results in patients with low levels of viremia. Moreover, anti-HEV IgM positivity is not a reliable indicator for distinguishing between acute and resolved infections given the ability of this antibody to persist several months after a resolved infection. Our study aims were to assess HEV IgG avidity for diagnosing acute and resolved infections, regardless of the anti-HEV IgM serostatus, and examine assay reliability when evaluating different genotype 3 (GT3) HEV subtypes. Patient serum samples (n = 104) were tested for HEV IgG avidity by utilizing the DIA.PRO kit on a DSX automated instrument. Among patients identified with acute HEV infections, 32 were infected with GT3: GT3c (n = 5), GT3e (n = 8), 3f (n = 17) and GT3-unsubtyped (n = 2). Avidity sensitivity was 91.2% and specificity was 100%. For patients with long-lasting anti-HEV IgM persistence, an Avidity Index >70% was observed. Thus, the DIA.PRO avidity assay may be utilized to distinguish between recently acquired and resolved HEV GT3 infections. However, for equivocal results (Avidity Index > 40-70%), HEV RNA molecular testing will be required to confirm a recent infection.
Keywords: HEV RNA; HEV acute hepatitis; HEV genotype 3; IgG avidity test; IgM; hepatitis E virus.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- GBD 2013 Mortality and Causes of Death Collaborators Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385:117–171. doi: 10.1016/S0140-6736(14)61682-2. - DOI - PMC - PubMed
-
- Smith D.B., Izopet J., Nicot F., Simmonds P., Jameel S., Meng X.J., Norder H., Okamoto H., van der Poel W.H.M., Reuter G., et al. Update: Proposed reference sequences for subtypes of hepatitis E virus (species Orthohepevirus A) J. Gen. Virol. 2020;101:692–698. doi: 10.1099/jgv.0.001435. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
