

Associations between post-stroke motor and cognitive function: a cross-sectional study
- PMID: 33546620
- PMCID: PMC7863272
- DOI: 10.1186/s12877-021-02055-7
Associations between post-stroke motor and cognitive function: a cross-sectional study
Abstract
Background: Motor and cognitive impairments are frequently observed following stroke, but are often managed as distinct entities, and there is little evidence regarding how they are related. The aim of this study was to describe the prevalence of concurrent motor and cognitive impairments 3 months after stroke and to examine how motor performance was associated with memory, executive function and global cognition.
Methods: The Norwegian Cognitive Impairment After Stroke (Nor-COAST) study is a prospective multicentre cohort study including patients hospitalized with acute stroke between May 2015 and March 2017. The National Institutes of Health Stroke Scale (NIHSS) was used to measure stroke severity at admission. Level of disability was assessed by the Modified Rankin Scale (mRS). Motor and cognitive functions were assessed 3 months post-stroke using the Montreal Cognitive Assessment (MoCA), Trail Making Test Part B (TMT-B), 10-Word List Recall (10WLR), Short Physical Performance Battery (SPPB), dual-task cost (DTC) and grip strength (Jamar®). Cut-offs were set according to current recommendations. Associations were examined using linear regression with cognitive tests as dependent variables and motor domains as covariates, adjusted for age, sex, education and stroke severity.
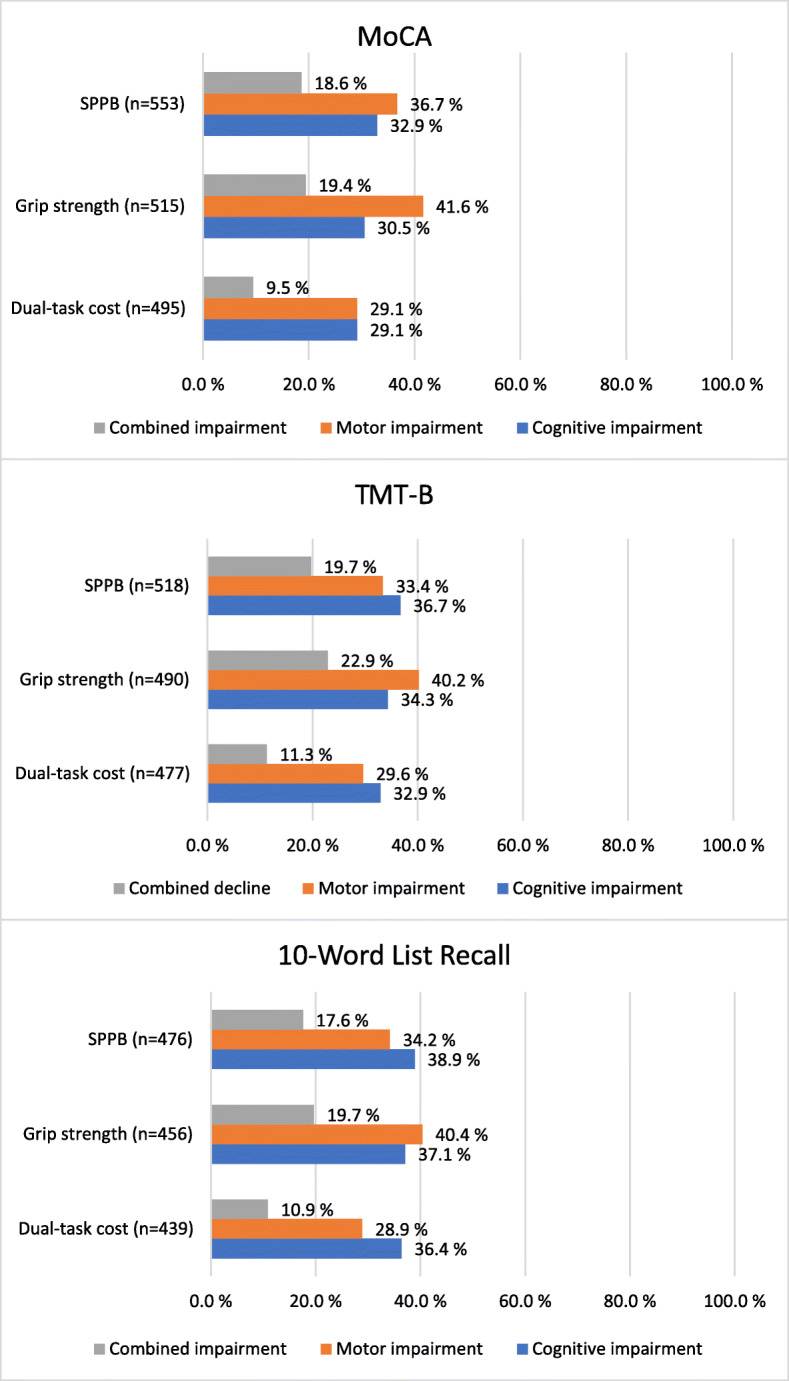
Results: Of 567 participants included, 242 (43%) were women, mean (SD) age was 72.2 (11.7) years, 416 (75%) had an NIHSS score ≤ 4 and 475 (84%) had an mRS score of ≤2. Prevalence of concurrent motor and cognitive impairment ranged from 9.5% for DTC and 10WLR to 22.9% for grip strength and TMT-B. SPPB was associated with MoCA (regression coefficient B = 0.465, 95%CI [0.352, 0.578]), TMT-B (B = -9.494, 95%CI [- 11.726, - 7.925]) and 10WLR (B = 0.132, 95%CI [0.054, 0.211]). Grip strength was associated with MoCA (B = 0.075, 95%CI [0.039, 0.112]), TMT-B (B = -1.972, 95%CI [- 2.672, - 1.272]) and 10WLR (B = 0.041, 95%CI [0.016, 0.066]). Higher DTC was associated with more time needed to complete TMT-B (B = 0.475, 95%CI [0.075, 0.875]) but not with MoCA or 10WLR.
Conclusion: Three months after suffering mainly minor strokes, 30-40% of participants had motor or cognitive impairments, while 20% had concurrent impairments. Motor performance was associated with memory, executive function and global cognition. The identification of concurrent impairments could be relevant for preventing functional decline.
Trial registration: ClinicalTrials.gov Identifier: NCT02650531 .
Keywords: Cognitive function; Function; Motor function; Stroke.
Conflict of interest statement
ABK and IS have been investigators in the drug trial Boehringer-Ingelheim 1346.0023, and ABK has also been an investigator for Roche BN29553. The remaining authors declare no conflicts interest.
Figures

References
-
- Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2197–2223. doi: 10.1016/S0140-6736(12)61689-4. - DOI - PubMed
-
- Fjærtoft H, Indredavik B, Mørch B, Phan A, Skogseth-Stephani R, Varmdal T. Årsrapport 2018, Norsk Hjerneslagregister. 2019.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
