

Implementing genomic screening in diverse populations
- PMID: 33546753
- PMCID: PMC7863616
- DOI: 10.1186/s13073-021-00832-y
Implementing genomic screening in diverse populations
Abstract
Background: Population-based genomic screening has the predicted ability to reduce morbidity and mortality associated with medically actionable conditions. However, much research is needed to develop standards for genomic screening and to understand the perspectives of people offered this new testing modality. This is particularly true for non-European ancestry populations who are vastly underrepresented in genomic medicine research. Therefore, we implemented a pilot genomic screening program in the BioMe Biobank in New York City, where the majority of participants are of non-European ancestry.
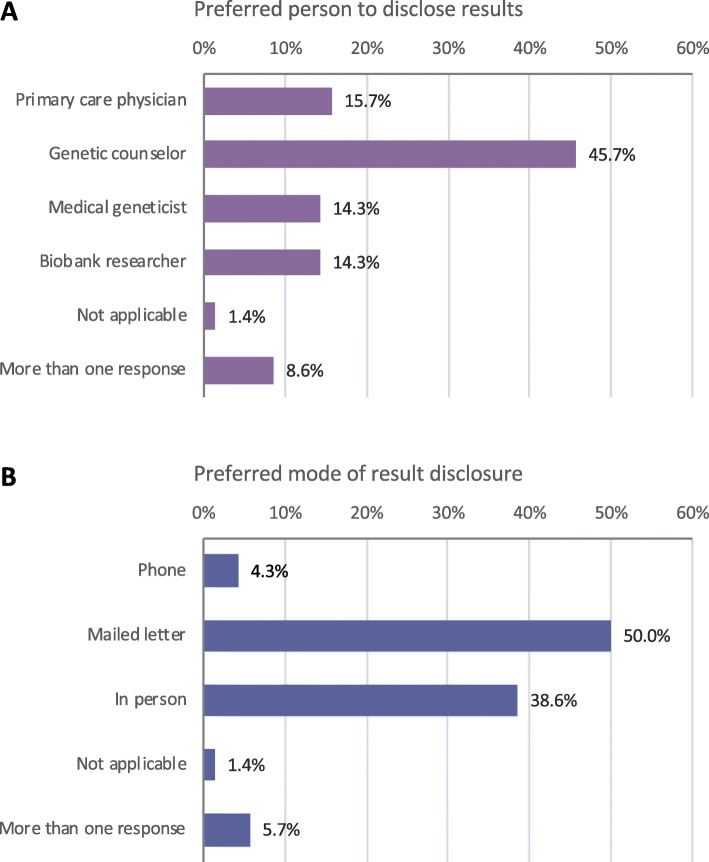
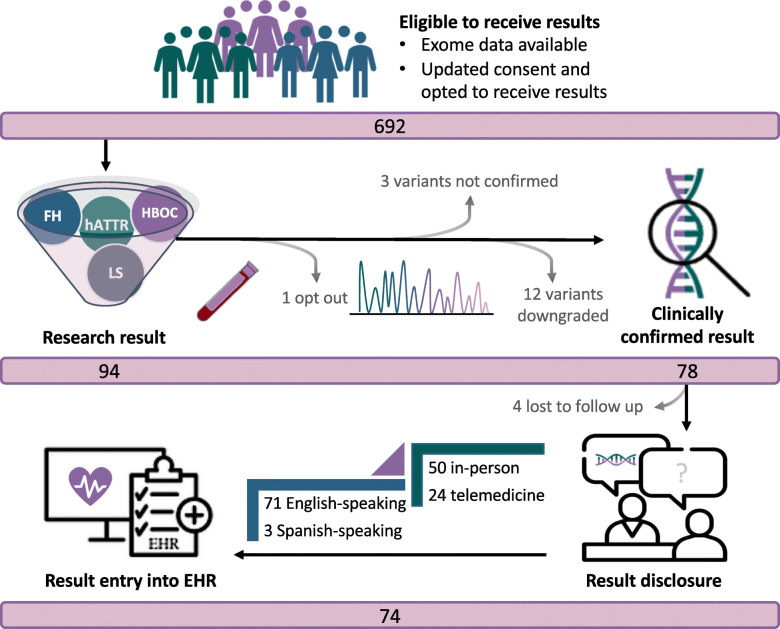
Methods: We initiated genomic screening for well-established genes associated with hereditary breast and ovarian cancer syndrome (HBOC), Lynch syndrome (LS), and familial hypercholesterolemia (FH). We evaluated and included an additional gene (TTR) associated with hereditary transthyretin amyloidosis (hATTR), which has a common founder variant in African ancestry populations. We evaluated the characteristics of 74 participants who received results associated with these conditions. We also assessed the preferences of 7461 newly enrolled BioMe participants to receive genomic results.
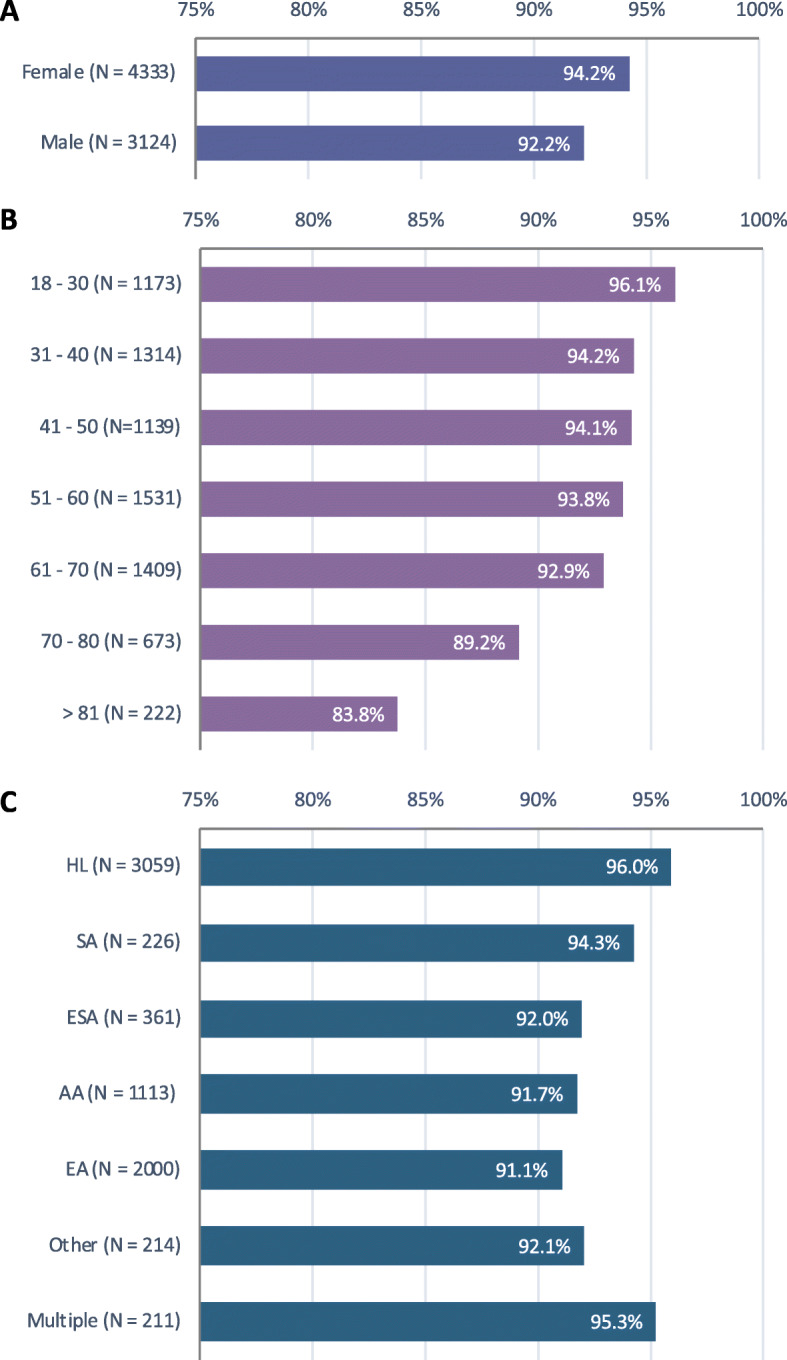
Results: In the pilot genomic screening program, 74 consented participants received results related to HBOC (N = 26), LS (N = 6), FH (N = 8), and hATTR (N = 34). Thirty-three of 34 (97.1%) participants who received a result related to hATTR were self-reported African American/African (AA) or Hispanic/Latinx (HL), compared to 14 of 40 (35.0%) participants who received a result related to HBOC, LS, or FH. Among the 7461 participants enrolled after the BioMe protocol modification to allow the return of genomic results, 93.4% indicated that they would want to receive results. Younger participants, women, and HL participants were more likely to opt to receive results.
Conclusions: The addition of TTR to a pilot genomic screening program meant that we returned results to a higher proportion of AA and HL participants, in comparison with genes traditionally included in genomic screening programs in the USA. We found that the majority of participants in a multi-ethnic biobank are interested in receiving genomic results for medically actionable conditions. These findings increase knowledge about the perspectives of diverse research participants on receiving genomic results and inform the broader implementation of genomic medicine in underrepresented patient populations.
Conflict of interest statement
N.S.A-H. was previously employed by Regeneron Pharmaceuticals and has received a speaker honorarium from Genentech. E.E.K. has received speaker honoraria from Illumina and Regeneron Pharmaceuticals. The remaining authors declare no competing interests.
Figures
References
-
- Grzymski JJ, Elhanan G, Morales Rosado JA, Smith E, Schlauch KA, Read R, et al. Population genetic screening efficiently identifies carriers of autosomal dominant diseases. Nat Med. 2020;26:1235–39. - PubMed
-
- Tier 1 genomics applications and their importance to public health | CDC 2019 [updated 2019/4/2. Available from: https://www.cdc.gov/genomics/implementation/toolkit/tier1.htm.
-
- Abul-Husn NS, Manickam K, Jones LK, Wright EA, Hartzel DN, Gonzaga-Jauregui C, et al. Genetic identification of familial hypercholesterolemia within a single U.S. health care system. Science. 2016;354(6319):aaf7000. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
