

Pulsatile ventricular assist device as a bridge to transplant for the early high-risk single-ventricle physiology
- PMID: 33546851
- PMCID: PMC8767640
- DOI: 10.1016/j.jtcvs.2020.09.071
Pulsatile ventricular assist device as a bridge to transplant for the early high-risk single-ventricle physiology
Abstract
Background: The use of ventricular assist devices (VADs) as a bridge-to-transplant in patients with single-ventricle physiology post-stage one palliation has been associated with poor outcomes. We describe our center's successful experience in the use of paracorporeal pulsatile VADs in the palliation of high-risk single ventricle physiology before or after the first stage of palliation with an impetus on pre-palliation implant.
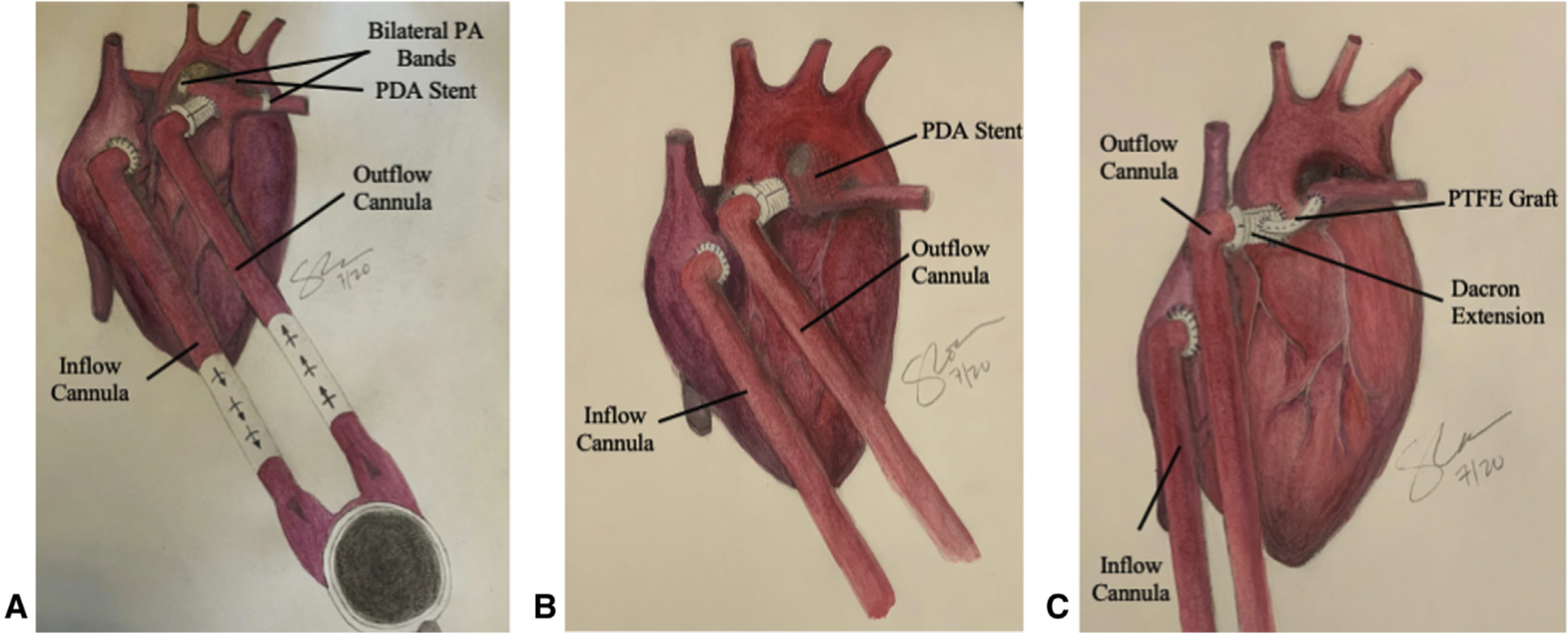
Methods: This is a single-center retrospective review of univentricular patients implanted with the Berlin Heart EXCOR VAD. Our center's approach includes early implantation of the Berlin Heart EXCOR with common atrial cannulation, a cardiac index between 3.5 and 5 L/min/m2, and a bivalirudin-based anticoagulation regimen. Patient-related data were collected postimplant at week 1 and months 1, 2, and 3. Post-transplant data, including neurological outcomes, were collected.
Results: Nine patients were supported. Survival to discharge post-transplant was 83% (5/6) in patients bridged-to-transplant and 33% (1/3) in patients bridged-to-decision. Six patients had no previous palliation. Median hospital stay before implantation was 111 days for nonsurvivors versus 20 days for survivors. The need for extracorporeal membrane oxygenation and cardiopulmonary resuscitation in nonsurvivors versus survivors was 1 in 3 versus 1 in 6 and 2 in 3 versus 1 in 6, respectively. There were no major central nervous system complications except for 1 significant hemorrhagic event. The pediatric overall performance category score on follow-up was normal to mild disability in 83% of survivors. Limitations include hemolysis and intermittent periods of infection and/or inflammation.
Conclusions: The use of pulsatile paracorporeal VADs is a feasible option as a bridge-to-transplant in the peri-stage one high-risk single ventricle.
Keywords: failing high-risk peri–stage-one single ventricle physiology; heart transplantation; mechanical circulatory support; pulsatile paracorporeal VAD.
Copyright © 2021. Published by Elsevier Inc.
Conflict of interest statement
Conflict of Interest Statement
The authors reported no conflicts of interest.
The
Figures




Comment in
-
Commentary: How to VAD to avoid BAD in high-risk single ventricle.J Thorac Cardiovasc Surg. 2021 Aug;162(2):414-415. doi: 10.1016/j.jtcvs.2020.09.117. Epub 2020 Oct 3. J Thorac Cardiovasc Surg. 2021. PMID: 33131889 No abstract available.
-
Commentary: Ventricular assist device support in an early infancy with single ventricle: Transformation from salvage to elective.J Thorac Cardiovasc Surg. 2021 Aug;162(2):416-417. doi: 10.1016/j.jtcvs.2020.10.045. Epub 2020 Oct 17. J Thorac Cardiovasc Surg. 2021. PMID: 33168164 No abstract available.
-
Commentary: Promise with pulsatility? Early bridging of high-risk patients with single-ventricle physiology with a ventricular assist device.J Thorac Cardiovasc Surg. 2021 Aug;162(2):415-416. doi: 10.1016/j.jtcvs.2020.09.079. Epub 2020 Sep 29. J Thorac Cardiovasc Surg. 2021. PMID: 34279228 No abstract available.
References
-
- Weinstein S, Bello R, Pizarro C, Fynn-Thompson F, Kirklin J, Guleserian K, et al. The use of the Berlin Heart EXCOR in patients with functional single ventricle. J Thorac Cardiovasc Surg. 2014;147:697–704. - PubMed
-
- Pearce FB, Kirklin JK, Holman WL, Barrett CS, Romp RL, Lau YR. Successful cardiac transplant after Berlin Heart bridge in a single ventricle heart: use of aortopulmonary shunt as a supplementary source of pulmonary blood flow. J Thorac Cardiovasc Surg. 2009;137:e40–2. - PubMed
-
- Conway J, St Louis J, Morales DLS, Law S, Tjossem C, Humpl T. Delineating survival outcomes in children <10 kg bridged to transplant or recovery with the Berlin Heart EXCOR ventricular assist device. JACC Heart Fail. 2015;3:70–7. - PubMed
-
- Gazit AZ, Petrucci O, Manning P, Shepard M, Baltagi S, Simpson K, et al. A novel surgical approach to mechanical circulatory support in univentricular infants. Ann Thorac Surg. 2017;104:1630–6. - PubMed
-
- Philip J, Lopez-colon D, Samraj RS, Kaliki G, Irwin MV, Pietra BA, et al. End-organ recovery post-ventricular assist device can prognosticate survival. J Crit Care. 2018;44:57–62. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
