

Sudden onset peripheral visual deficit secondary to retinal artery spasm in Raynaud's phenomenon
- PMID: 33547102
- PMCID: PMC7871241
- DOI: 10.1136/bcr-2020-239954
Sudden onset peripheral visual deficit secondary to retinal artery spasm in Raynaud's phenomenon
Abstract
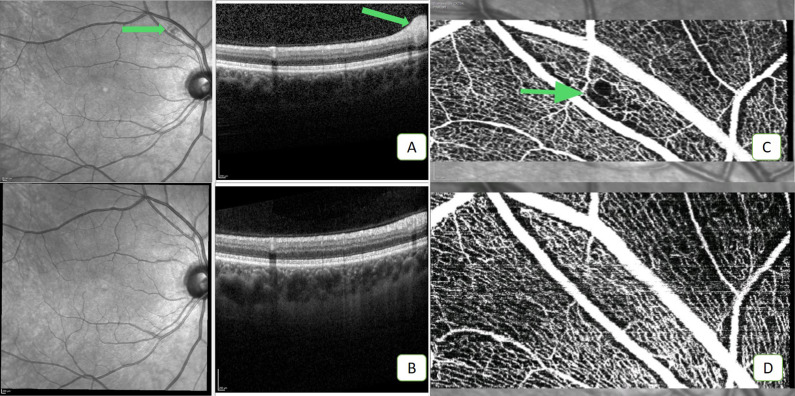
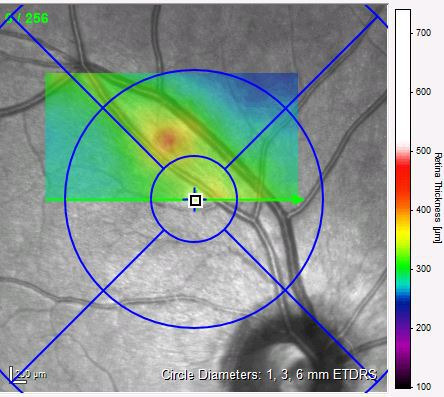
A 32-year-old doctor, who has a medical history of primary Raynaud's disease and previous scotomas, presented to eye clinic with sudden onset blurring of vision (infero-nasally) with no other associated symptoms. The patient had good visual acuity bilaterally (6/6) and no anterior chamber activity or conjunctival hyperaemia. Findings consistent with a nerve fibre layer infarct were noted in the right eye, with unremarkable examination of the left eye. Optical coherence tomography (OCT) and optical coherence tomography angiography (OCTA) images were obtained, which showed an area of capillary shut down in keeping with a nerve fibre layer lesion. Previous literature pertaining to similar symptoms is sparse with symptoms such as migraines, epilepsy and visual loss being stated. This case provides further evidence of Raynaud's associated retinal artery spasm, with complete resolution at 4 weeks. We also demonstrate the accessibility of OCT and more importantly OCTA for investigation of sudden onset visual deficit.
Keywords: ophthalmology; retina; rheumatology.
© BMJ Publishing Group Limited 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical