

Optimal Phosphate Control Related to Coronary Artery Calcification in Dialysis Patients
- PMID: 33547218
- PMCID: PMC7920180
- DOI: 10.1681/ASN.2020050598
Optimal Phosphate Control Related to Coronary Artery Calcification in Dialysis Patients
Abstract
Background: In patients on maintenance dialysis, cardiovascular mortality risk is remarkably high, which can be partly explained by severe coronary artery calcification (CAC). Hyperphosphatemia has been reported to be associated with the severity of CAC. However, the optimal phosphate range in patients on dialysis remains unknown. This study was planned to compare the effects on CAC progression of two types of noncalcium-based phosphate binders and of two different phosphate target ranges.
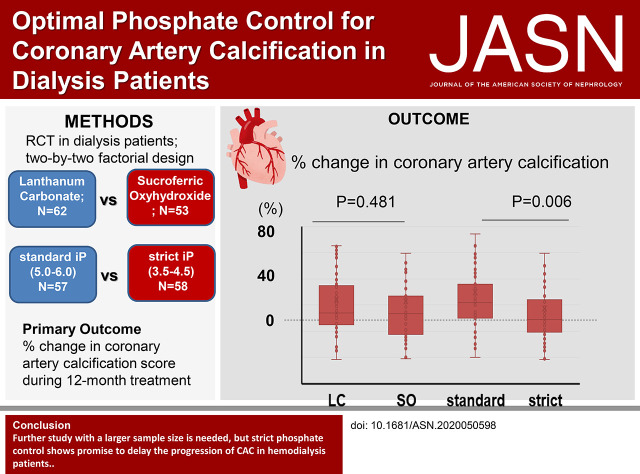
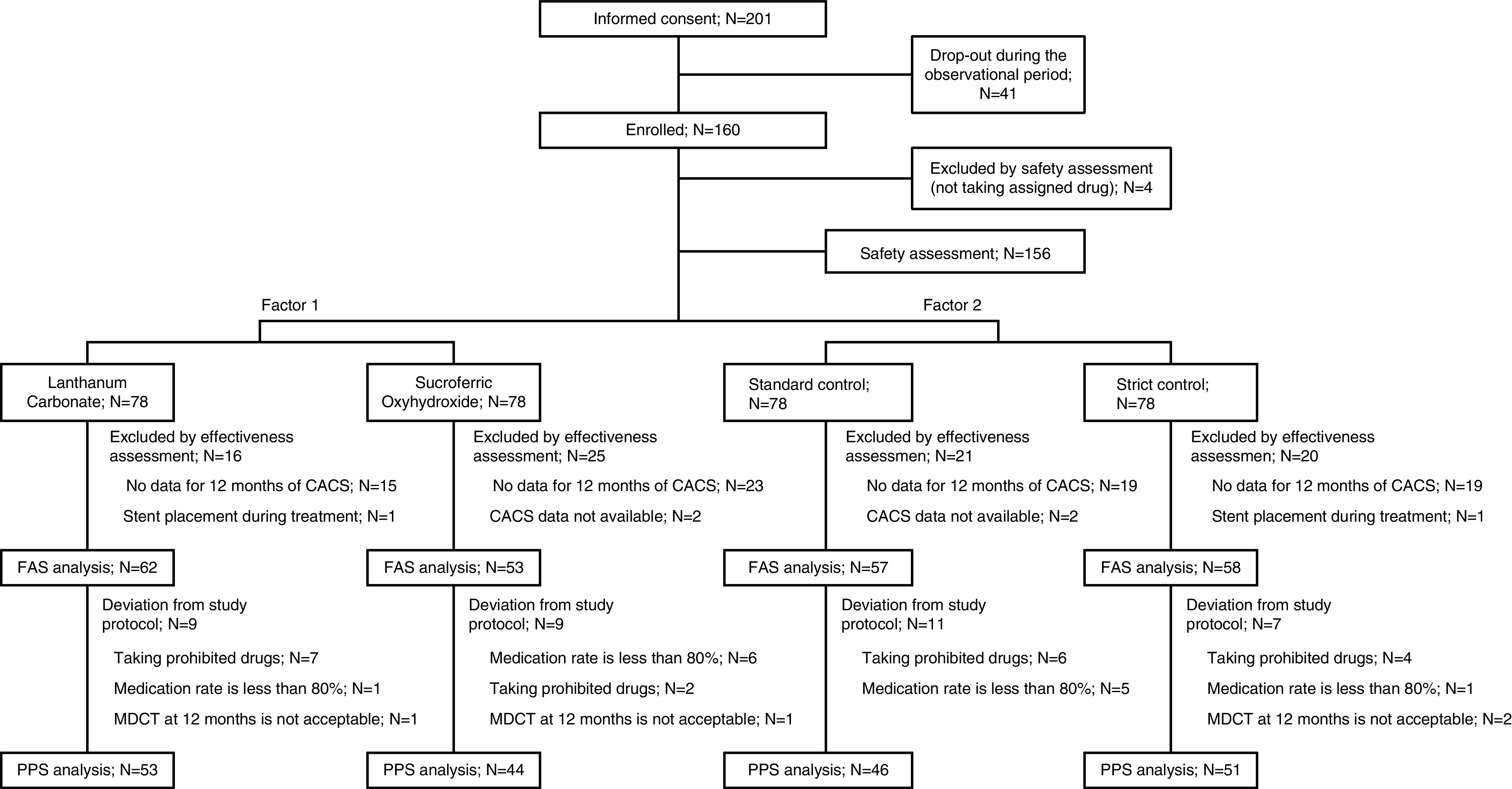
Methods: We conducted a randomized, open-label, multicenter, interventional trial with a two by two factorial design. A total of 160 adults on dialysis were enrolled and randomized to the sucroferric oxyhydroxide or lanthanum carbonate group, with the aim of reducing serum phosphate to two target levels (3.5-4.5 mg/dl in the strict group and 5.0-6.0 mg/dl in the standard group). The primary end point was percentage change in CAC scores during the 12-month treatment.
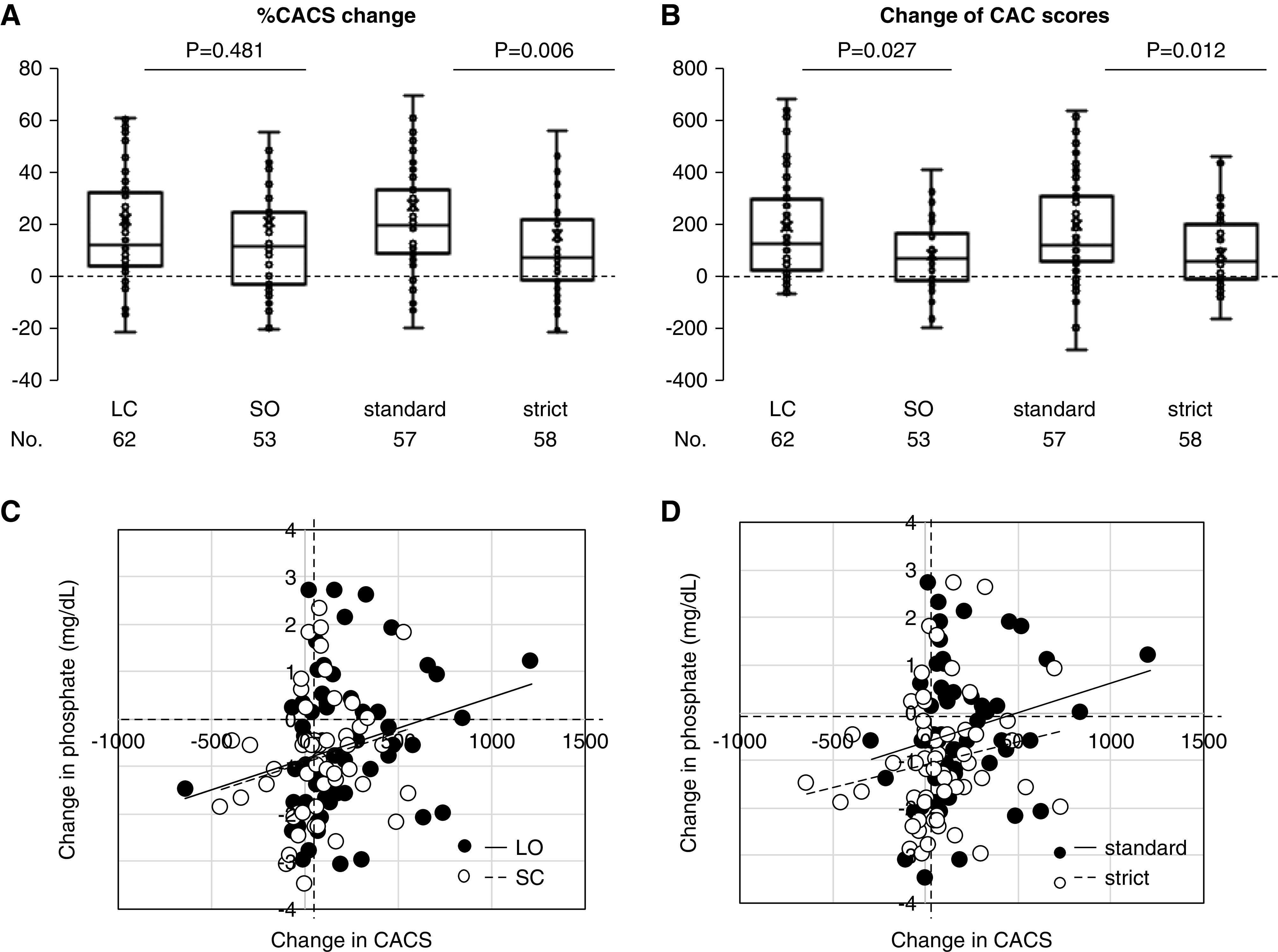
Results: The full analysis set included 115 patients. We observed no significant difference in percentage change in CAC scores between the lanthanum carbonate group and the sucroferric oxyhydroxide group. On the other hand, percentage change in CAC scores in the strict group (median of 8.52; interquartile range, -1.0-23.9) was significantly lower than that in the standard group (median of 21.8; interquartile range, 10.0-36.1; P=0.006). This effect was pronounced in older (aged 65-74 years) versus younger (aged 20-64 years) participants (P value for interaction =0.003). We observed a similar finding for the absolute change in CAC scores.
Conclusions: Further study with a larger sample size is needed, but strict phosphate control shows promise for delaying progression of CAC in patients undergoing maintenance hemodialysis.
Clinical trial registry name and registration number: Evaluate the New Phosphate Iron-Based Binder Sucroferric Oxyhydroxide in Dialysis Patients with the Goal of Advancing the Practice of EBM (EPISODE), jRCTs051180048.
Keywords: coronary calcification; dialysis; hyperphosphatemia; phosphate binders.
Copyright © 2021 by the American Society of Nephrology.
Figures

Comment in
-
In Search of the Optimal Target for Phosphate Control: Episode 1.J Am Soc Nephrol. 2021 Mar;32(3):526-528. doi: 10.1681/ASN.2021010027. Epub 2021 Feb 5. J Am Soc Nephrol. 2021. PMID: 33547217 Free PMC article. No abstract available.
References
-
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Update Work Group: KDIGO 2017. clinical practice guideline update for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Available at: https://kdigo.org/wp-content/uploads/2017/02/2017-KDIGO-CKD-MBD-GL-Updat.... Accessed March 14, 2020 - PMC - PubMed
-
- Block GA, Raggi P, Bellasi A, Kooienga L, Spiegel DM: Mortality effect of coronary calcification and phosphate binder choice in incident hemodialysis patients. Kidney Int 71: 438–441, 2007 - PubMed
-
- Cannata-Andía JB, Fernández-Martín JL, Locatelli F, London G, Gorriz JL, Floege J, et al.: Use of phosphate-binding agents is associated with a lower risk of mortality. Kidney Int 84: 998–1008, 2013 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
