

Integrative molecular characterization of sarcomatoid and rhabdoid renal cell carcinoma
- PMID: 33547292
- PMCID: PMC7865061
- DOI: 10.1038/s41467-021-21068-9
Integrative molecular characterization of sarcomatoid and rhabdoid renal cell carcinoma
Abstract
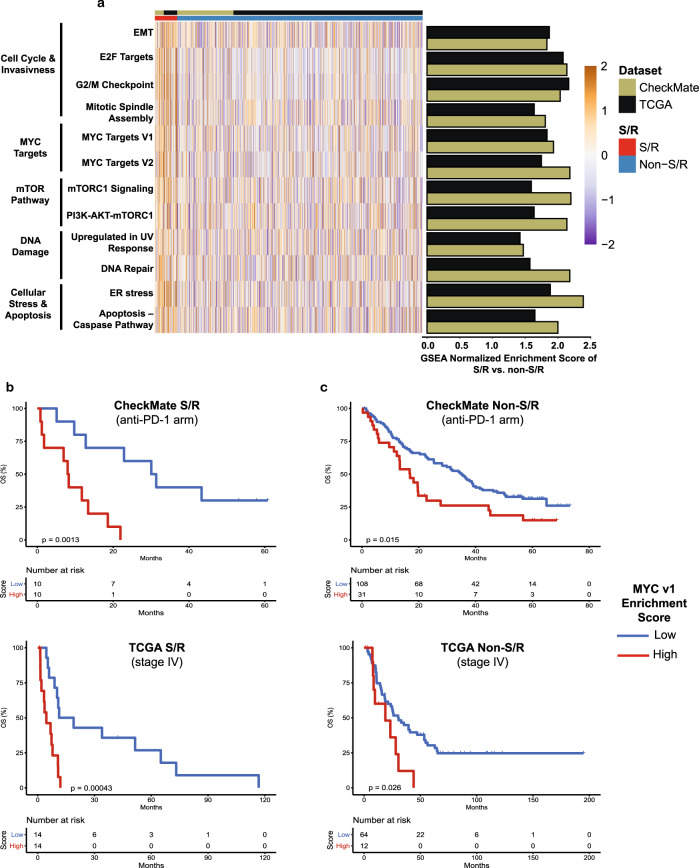
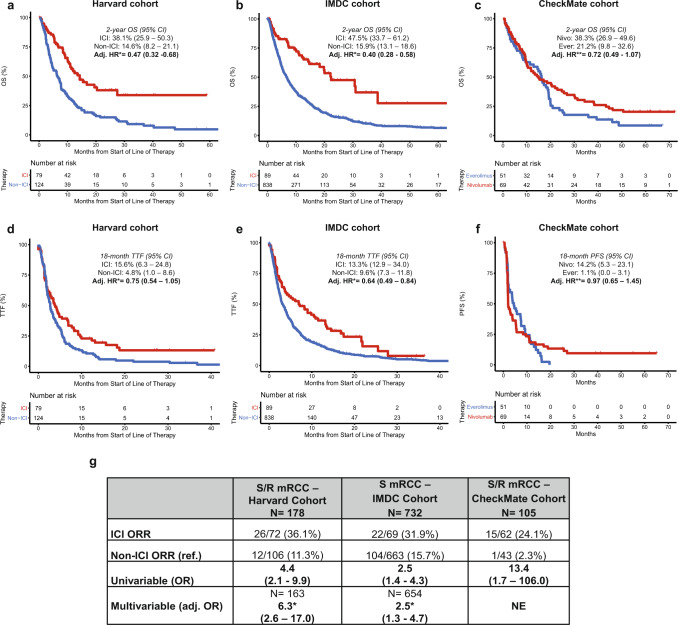
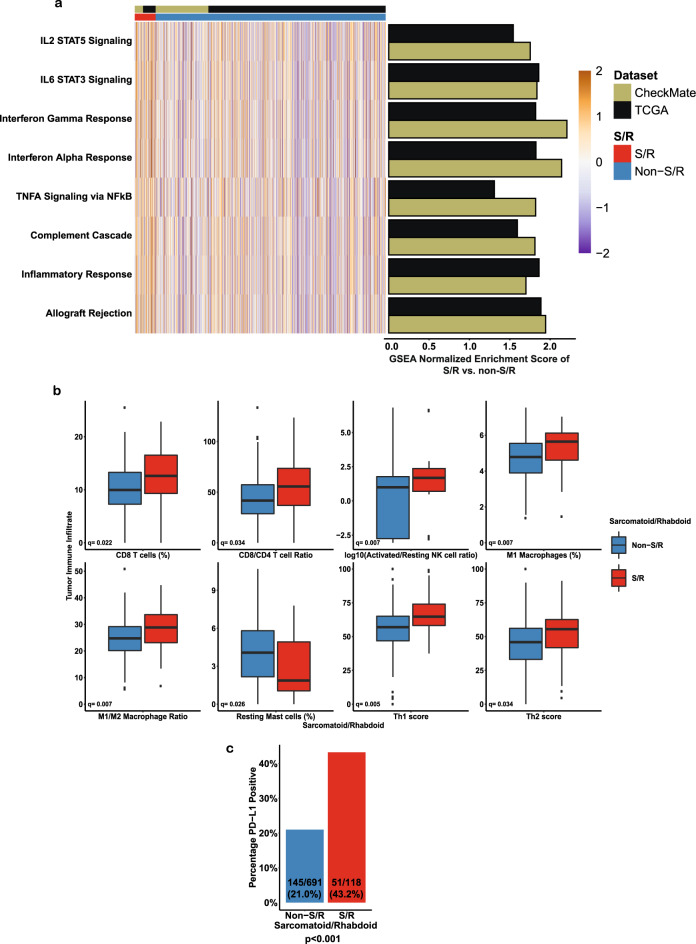
Sarcomatoid and rhabdoid (S/R) renal cell carcinoma (RCC) are highly aggressive tumors with limited molecular and clinical characterization. Emerging evidence suggests immune checkpoint inhibitors (ICI) are particularly effective for these tumors, although the biological basis for this property is largely unknown. Here, we evaluate multiple clinical trial and real-world cohorts of S/R RCC to characterize their molecular features, clinical outcomes, and immunologic characteristics. We find that S/R RCC tumors harbor distinctive molecular features that may account for their aggressive behavior, including BAP1 mutations, CDKN2A deletions, and increased expression of MYC transcriptional programs. We show that these tumors are highly responsive to ICI and that they exhibit an immune-inflamed phenotype characterized by immune activation, increased cytotoxic immune infiltration, upregulation of antigen presentation machinery genes, and PD-L1 expression. Our findings build on prior work and shed light on the molecular drivers of aggressivity and responsiveness to ICI of S/R RCC.
Conflict of interest statement
Z.B.: reported nonfinancial support from Bristol-Myers Squibb and Genentech/ImCore. D.A.B. reported nonfinancial support from, Bristol-Myers Squibb, and personal fees from Octane Global, Defined Health, Dedham Group, Adept Field Solutions, Slingshot Insights, Blueprint Partnerships, Charles River Associates, Trinity Group, and Insight Strategy, outside of the submitted work. S.A.S. reported nonfinancial support from Bristol-Myers Squibb, and equity in 152 Therapeutics outside the submitted work. X.G: Research Support to Institution: Exelixis. X.X.W: Research Support: BMS. B.A.M is a consultant for Bayer, Astellas, Astra Zeneca, Seattle Genetics, Exelixis, Nektar, Pfizer, Janssen, Genentech and EMD Serono. He received research support to Dana Farber Cancer Institute (DFCI) from Bristol Myers Squibb, Calithera, Exelixis, Seattle Genetics. L.C.H reports consulting fees from Genentech, Dendreon, Pfizer, Medivation/Astellas, Exelixis, Bayer, Kew Group, Corvus, Merck, Novartis, Michael J Hennessy Associates (Healthcare Communications Company and several brands such as OncLive and PER), Jounce, EMD Serrano, and Ology Medical Education; Research funding from Bayer, Sotio, Bristol-Myers Squib, Merck, Takeda, Dendreon/Valient, Jannsen, Medivation/Astellas, Genentech, Pfizer, Endocyte (Novartis), and support for research travel from Bayer and Genentech. M.B.A: Advisory Board participation: BMS, Merck, Novartis, Arrowhead, Pfizer, Galactone, Werewolf, Fathom, Pneuma, Leads BioPharma; Consultant: BMS, Merck, Novartis, Pfizer, Genentech-Roche, Exelixis, Eisai, Aveo, Array, AstraZeneca, Ideera, Aduro, ImmunoCore, Boehringer-Ingelheim, Iovance, Newlink, Pharma, Surface, Alexion, Acceleron, Cota, Amgen; Research Support to institution: BMS, Merck, Pfizer, Genentech. C.J.W.: Co-founder of Neon Therapeutics, and is a member of its SAB. Receives research funding from Pharmacyclics. T.H.H: Advisory board participation: Surface Therapeutics, Exelixis, Genentech, Pfizer, Ipsen, Cardinal Health; research support-Novartis. D.F.M reports a consulting/advisory role for Bristol-Myers Squibb, Merck, Roche/Genentech, Pfizer, Exelixis, Novartis, Eisai, X4 Pharmaceuticals, and Array BioPharma; and reports that his home institution receives research funding from Prometheus Laboratories. D.H: consulting or research funding from Pfizer, Novartis, BMS, Ipsen, Exelixis, and Merck. S.R.V.: consultant for MPM Capital and has consulted for Vida Ventures. S.S: Research support to Institution: Bristol-Myers Squibb, AstraZeneca, Novartis, Exelixis; Consultant: Merck, AstraZeneca, Bristol-Myers Squibb, AACR, and NCI; royalties: Biogenex. E.M.V: Advisory/Consulting: Tango Therapeutics, Genome Medical, Invitae, Illumina, Ervaxx; Research support: Novartis, BMS; Equity: Tango Therapeutics, Genome Medical, Syapse, Ervaxx, Microsoft; Travel reimbursement: Roche/Genentech; Patents: Institutional patents filed on ERCC2 mutations and chemotherapy response, chromatin mutations and immunotherapy response, and methods for clinical interpretation. T.K.C.: Research (Institutional and personal): Alexion, Analysis Group, AstraZeneca, Bayer, Bristol Myers-Squibb/ER Squibb and sons LLC, Calithera, Cerulean, Corvus, Eisai, Exelixis, F. Hoffmann-La Roche, Foundation Medicine Inc., Genentech, GlaxoSmithKline, Ipsen, Lilly, Merck, Novartis, Peloton, Pfizer, Prometheus Labs, Roche, Roche Products Limited, Sanofi/Aventis, Takeda, Tracon. Honoraria: Alexion, American Society of Medical Oncology, Analysis Group, AstraZeneca, Bayer, Bristol Myers-Squibb/ER Squibb and sons LLC, Cerulean, Clinical Care Options, Corvus, Eisai, EMD Serono, ESMO, Exelixis, F. Hoffmann-La Roche, Foundation Medicine Inc., Genentech, GlaxoSmithKline, Harborside Press, Heron Therapeutics, Inc (Healthcare Communications Company with several brands such as OnClive, PeerView and PER), Jansen Oncology, IQVIA, Ipsen, Kidney Cancer Journal, Lancet Oncology, Lilly Oncology, L-path, Medscape, Merck, Michael J. Hennessy (MJH) Associates, Navinata Healthcare, NCCN, NEJM, Novartis, Peloton, Pfizer, Platform Q, Practice, PrimeOncology, Prometheus Labs, Research to, Roche, Roche Products Limited, Sanofi/Aventis, Up-to-Date. Consulting or Advisory Role: Alexion, Analysis Group, AstraZeneca, Bayer, Bristol Myers-Squibb/ER Squibb and sons LLC, Cerulean, Corvus, Eisai, EMD Serono, Exelixis, Foundation Medicine Inc., Genentech, GlaxoSmithKline, Heron Therapeutics, Infinity Pharma, Ipsen, Lilly, Lilly Ventures, Merck, NCCN, Novartis, Peloton, Pfizer, Pionyr, Prometheus Labs, Roche, Sanofi/Aventis, Surface Oncology, Tempest, Up-to-Date. Stock ownership: Pionyr, Tempest. No leadership or employment in for-profit companies. Other present or past leadership roles: Director of GU Oncology Division at Dana-Farber and past president of Medical Staff at Dana-Farber), member of NCCN Kidney panel and the GU Steering Committee, past chairman of the Kidney Cancer Association Medical and Scientific Steering Committee), KidneyCan Advisory board, Kidney Cancer Research Summit co-chair (2019-), various ASCO/ESMO roles on educational and scientific committees. Patents filed, royalties or other intellectual properties: related to biomarkers of immune checkpoint blockers, and circulating free methylated DNA Travel, accommodations, expenses, in relation to consulting, advisory roles, or honoraria. Medical writing and editorial assistance support may have been funded by Communications companies funded by pharmaceutical companies (e.g. ClinicalThinking, Envision Pharma Group, Fishawack Group of Companies, Health Interactions, Parexel, Oxford PharmaGenesis, pharmagenesis, and others). The institution (Dana-Farber Cancer Institute) may have received additional independent funding of drug companies or/and royalties potentially involved in research around the subject matter. CV provided upon request for scope of clinical practice and research. Mentored several non-US citizens on research projects with potential funding (in part) from non-US sources/Foreign Components. No speaker’s bureau.
Figures

Comment in
-
Characterizing sarcomatoid and rhabdoid RCC.Nat Rev Urol. 2021 Apr;18(4):189. doi: 10.1038/s41585-021-00446-4. Nat Rev Urol. 2021. PMID: 33686289 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
