

NLRC5/CITA expression correlates with efficient response to checkpoint blockade immunotherapy
- PMID: 33547395
- PMCID: PMC7865024
- DOI: 10.1038/s41598-021-82729-9
NLRC5/CITA expression correlates with efficient response to checkpoint blockade immunotherapy
Abstract
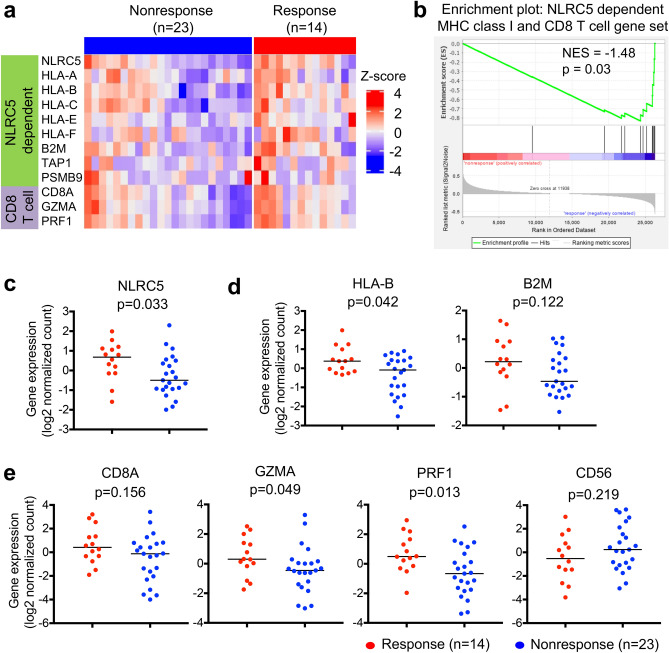
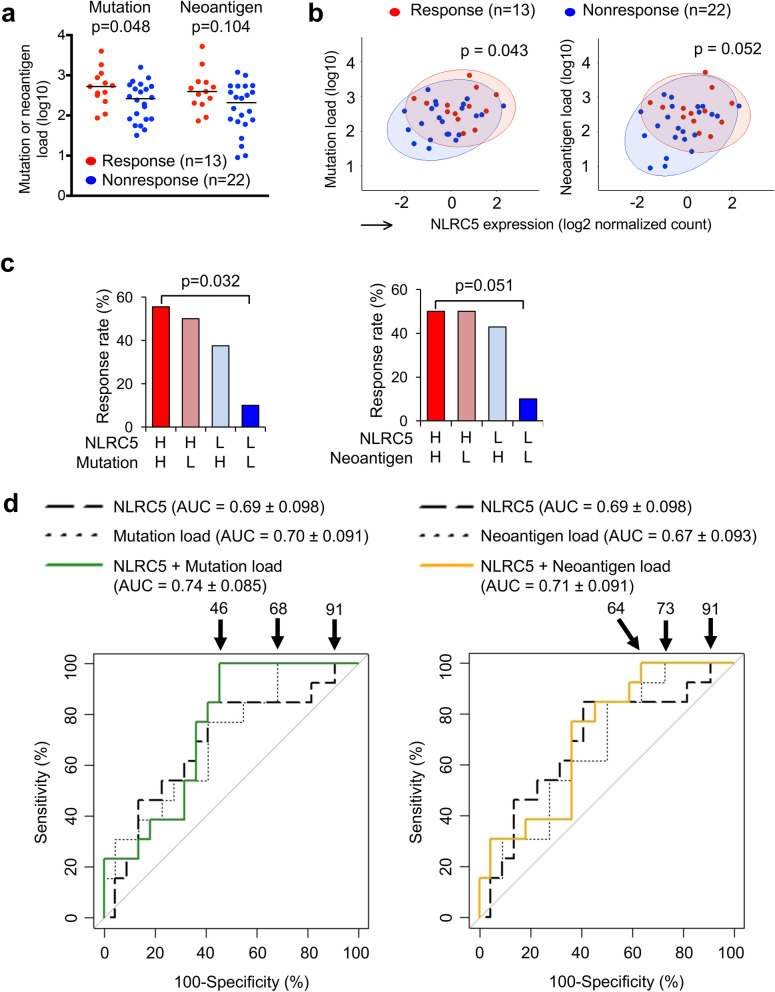
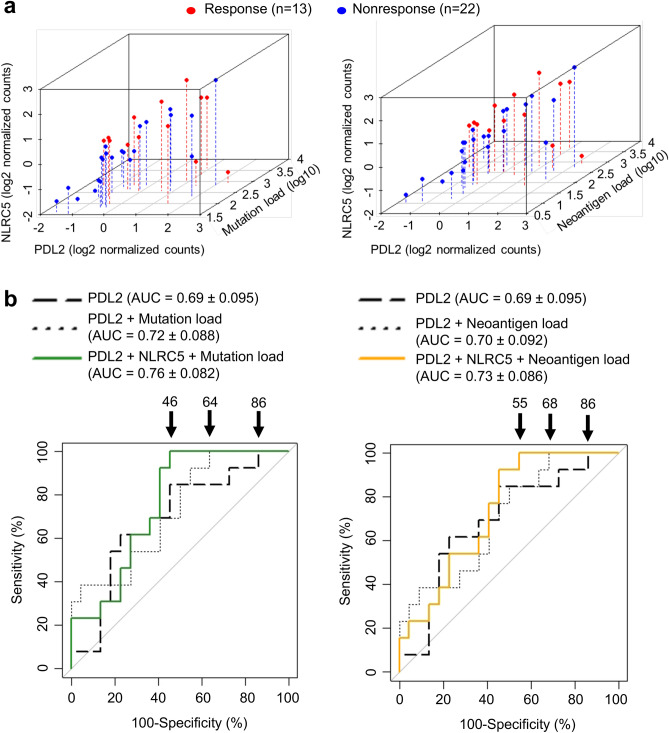
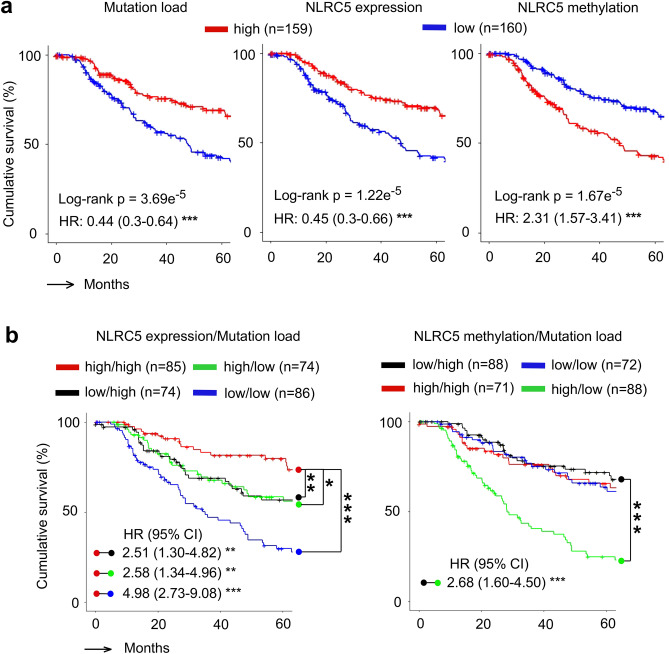
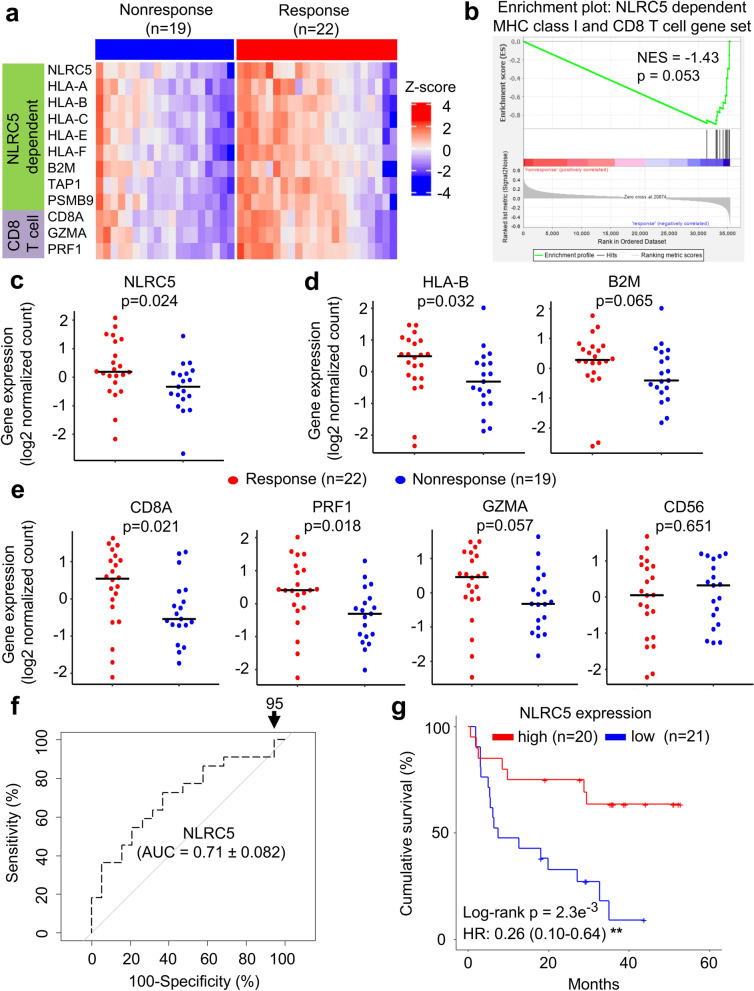
Checkpoint blockade-mediated immunotherapy is emerging as an effective treatment modality for multiple cancer types. However, cancer cells frequently evade the immune system, compromising the effectiveness of immunotherapy. It is crucial to develop screening methods to identify the patients who would most benefit from these therapies because of the risk of the side effects and the high cost of treatment. Here we show that expression of the MHC class I transactivator (CITA), NLRC5, is important for efficient responses to anti-CTLA-4 and anti-PD1 checkpoint blockade therapies. Melanoma tumors derived from patients responding to immunotherapy exhibited significantly higher expression of NLRC5 and MHC class I-related genes compared to non-responding patients. In addition, multivariate analysis that included the number of tumor-associated non-synonymous mutations, predicted neo-antigen load and PD-L2 expression was capable of further stratifying responders and non-responders to anti-CTLA4 therapy. Moreover, expression or methylation of NLRC5 together with total somatic mutation number were significantly correlated with increased patient survival. These results suggest that NLRC5 tumor expression, alone or together with tumor mutation load constitutes a valuable predictive biomarker for both prognosis and response to anti-CTLA-4 and potentially anti-PD1 blockade immunotherapy in melanoma patients.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
