

Predictive value of plasma proenkephalin and neutrophil gelatinase-associated lipocalin in acute kidney injury and mortality in cardiogenic shock
- PMID: 33547528
- PMCID: PMC7865050
- DOI: 10.1186/s13613-021-00814-8
Predictive value of plasma proenkephalin and neutrophil gelatinase-associated lipocalin in acute kidney injury and mortality in cardiogenic shock
Abstract
Background: Acute kidney injury (AKI) is a frequent form of organ injury in cardiogenic shock. However, data on AKI markers such as plasma proenkephalin (P-PENK) and neutrophil gelatinase-associated lipocalin (P-NGAL) in cardiogenic shock populations are lacking. The objective of this study was to assess the ability of P-PENK and P-NGAL to predict acute kidney injury and mortality in cardiogenic shock.
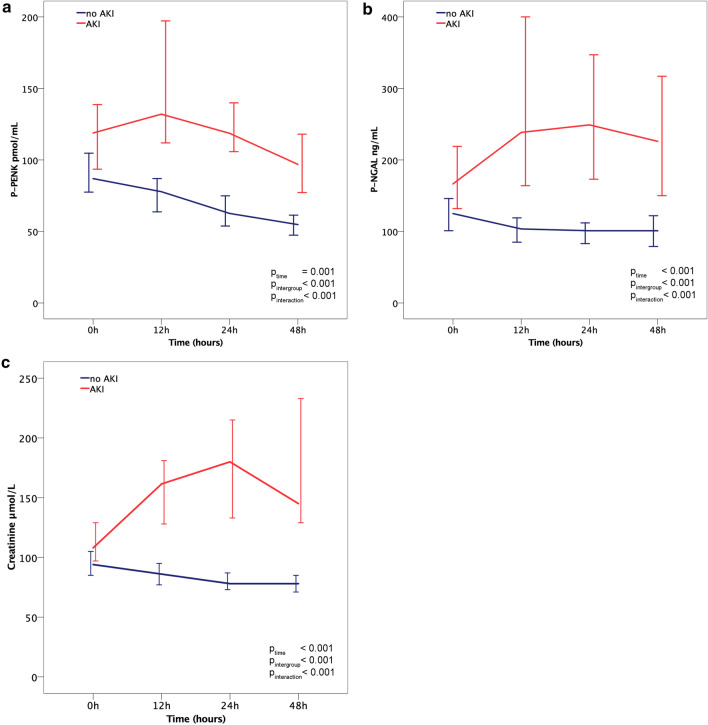
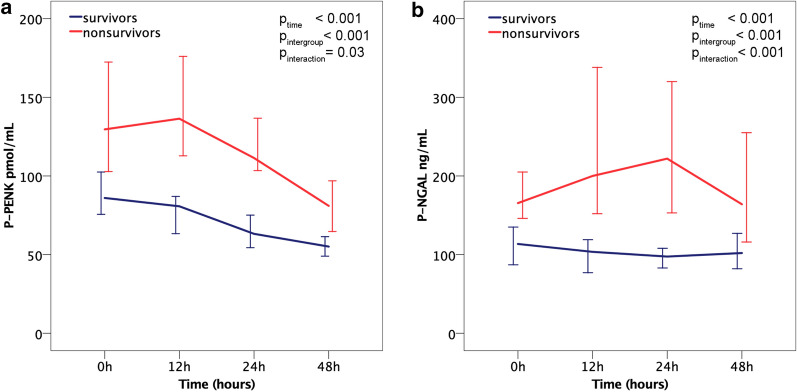
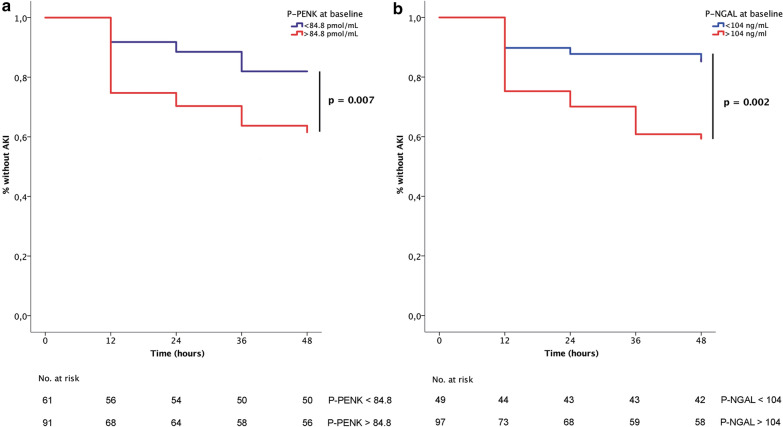
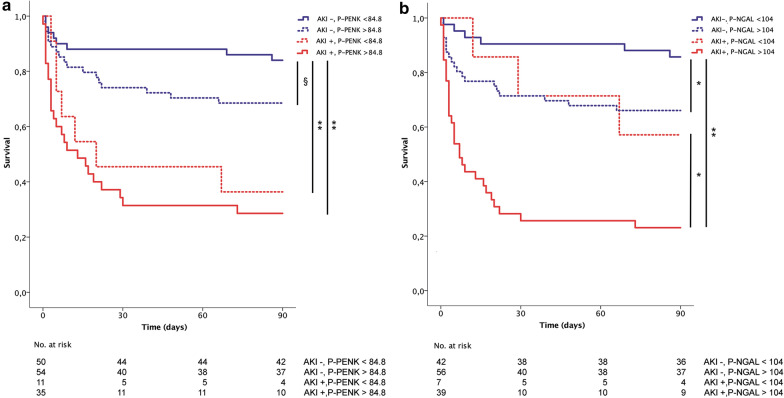
Results: P-PENK and P-NGAL were measured at different time points between baseline and 48 h in 154 patients from the prospective CardShock study. The outcomes assessed were AKI defined by an increase in creatinine within 48 h and all-cause 90-day mortality. Mean age was 66 years and 26% were women. Baseline levels of P-PENK and P-NGAL (median [interquartile range]) were 99 (71-150) pmol/mL and 138 (84-214) ng/mL. P-PENK > 84.8 pmol/mL and P-NGAL > 104 ng/mL at baseline were identified as optimal cut-offs for AKI prediction and independently associated with AKI (adjusted HRs 2.2 [95% CI 1.1-4.4, p = 0.03] and 2.8 [95% CI 1.2-6.5, p = 0.01], respectively). P-PENK and P-NGAL levels at baseline were also associated with 90-day mortality. For patients with oliguria < 0.5 mL/kg/h for > 6 h before study enrollment, 90-day mortality differed significantly between patients with low and high P-PENK/P-NGAL at baseline (5% vs. 68%, p < 0.001). However, the biomarkers provided best discrimination for mortality when measured at 24 h. Identified cut-offs of P-PENK24h > 105.7 pmol/L and P-NGAL24h > 151 ng/mL had unadjusted hazard ratios of 5.6 (95% CI 3.1-10.7, p < 0.001) and 5.2 (95% CI 2.8-9.8, p < 0.001) for 90-day mortality. The association remained significant despite adjustments with AKI and two risk scores for mortality in cardiogenic shock.
Conclusions: High levels of P-PENK and P-NGAL at baseline were independently associated with AKI in cardiogenic shock patients. Furthermore, oliguria before study inclusion was associated with worse outcomes only if combined with high baseline levels of P-PENK or P-NGAL. High levels of both P-PENK and P-NGAL at 24 h were found to be strong and independent predictors of 90-day mortality.
Trial registration: NCT01374867 at www.clinicaltrials.gov , registered 16 Jun 2011-retrospectively registered.
Keywords: AKI; Acute kidney injury; Cardiogenic shock; Mortality; NGAL; PENK; Proenkephalin; Prognosis.
Conflict of interest statement
VPH: advisory board fees from Roche Diagnostics, research grant from Abbott, speaker fees from Orion. KP: advisory board fees from Roche Diagnostics. JSC has consulted and received speaker fees, or advisory boards’ participation fees, or investigational grants for Abbott, Astra-Zeneca Pharmaceuticals, Bial, Boehringer Ingelheim, Menarini, Merck Serono, Merck Sharp & Dohme, Novartis, Orion, Pfizer, Sanofi, Servier and Vifor. AM: lecture fees from Novartis, Orion, and Abbott, research grants from Roche, consultant fees from Servier and Sanofi and fees as a member of the advisory board and/or steering committee from Cardiorentis, Adrenomed, Sphingotec, Sanofi, Roche, Abbott, and Bristol-Myers Squibb. JL: Speakers bureau and consultancy fees: Astra-Zeneca, Bayer, Boehringer-Ingelheim, Novartis, Orion, Pfizer, Roche Diagnostics, and ViforPharma. All other authors report that they have no relationships with industry to disclose.
Figures
References
-
- Tarvasmäki T, Haapio M, Mebazaa A, Sionis A, Silva-Cardoso J, Tolppanen H, et al. Acute kidney injury in cardiogenic shock: definitions, incidence, haemodynamic alterations, and mortality. Eur J Heart Fail. 2017;10:193–210. - PubMed
-
- Kellum JA, Lameire N, Aspelin P, Barsoum RS, Burdmann EA, Goldstein SL, et al. Kidney disease: Improving global outcomes (KDIGO) acute kidney injury work group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2:1–138. doi: 10.1038/kisup.2012.1. - DOI
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
