

Intrathecal dexamethasone therapy for febrile infection-related epilepsy syndrome
- PMID: 33547757
- PMCID: PMC7951105
- DOI: 10.1002/acn3.51308
Intrathecal dexamethasone therapy for febrile infection-related epilepsy syndrome
Abstract
Objective: Increasing reports suggest a role for immunological mechanisms in febrile infection-related epilepsy syndrome (FIRES). The objective of this study was to elucidate the efficacy and safety of intrathecal dexamethasone therapy (IT-DEX).
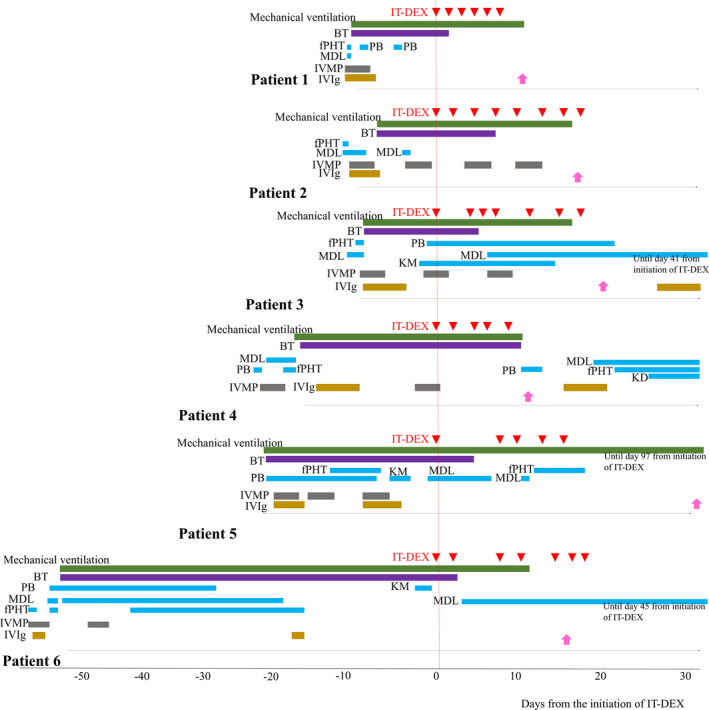
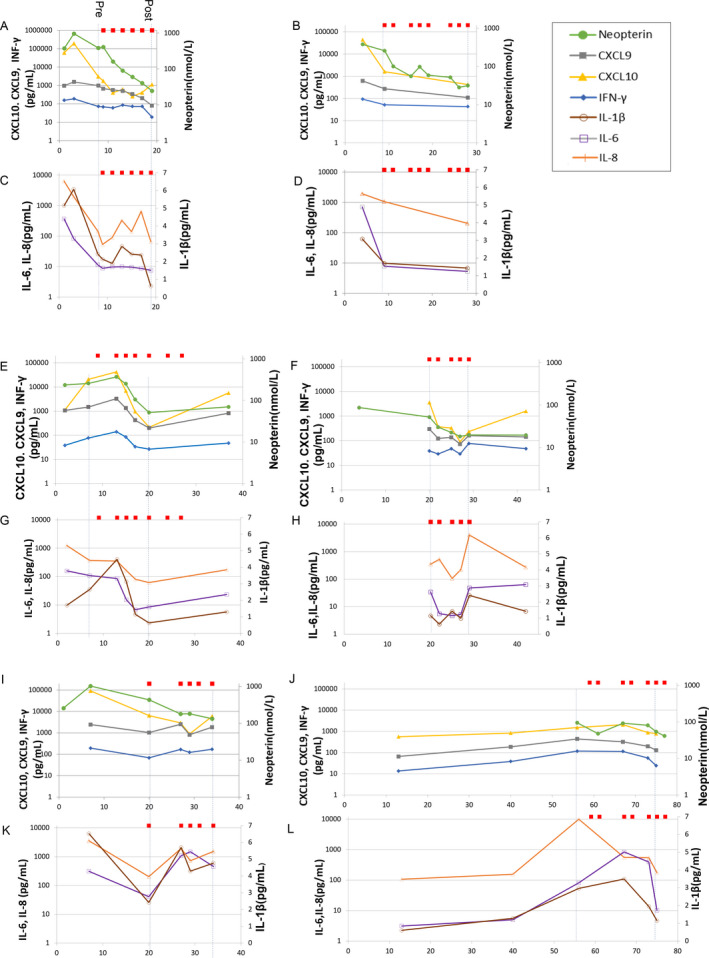
Methods: We assessed six pediatric patients with FIRES who were administered add-on IT-DEX in the acute (n = 5) and chronic (n = 1) phases. We evaluated clinical courses and prognosis. We measured cytokines/chemokines in cerebrospinal fluid (CSF) from FIRES patients at several points, including pre- and post-IT-DEX, and compared them with control patients with chronic epilepsy (n = 12, for cytokines/chemokines) or with noninflammatory neurological disease (NIND, n = 13, for neopterin).
Results: Anesthesia was weaned after a median of 5.5 days from IT-DEX initiation (n = 6). There was a positive correlation between the duration from the disease onset to the introduction of IT-DEX and the length of ICU stay and the duration of mechanical ventilation. No patient experienced severe adverse events. Seizure spreading and background activities on electroencephalography were improved after IT-DEX in all patients. The levels of CXCL10, CXCL9, IFN-γ, and neopterin at pre-IT-DEX were significantly elevated compared to levels in epilepsy controls, and CXCL10 and neopterin were significantly decreased post-IT-DEX, but were still higher compared to patients with chronic epilepsy. IL-6, IL-8, and IL-1β were significantly elevated before IT-DEX compared to epilepsy controls, though there was no significant decrease post-treatment.
Interpretation: IT-DEX represents a therapeutic option for patients with FIRES that could shorten the duration of the critical stage of the disease. The effect of IT-DEX on FIRES might include cytokine-independent mechanisms.
© 2021 The Authors. Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
None of the authors has any conflict of interest to disclose.
Figures

References
-
- van Baalen A, Hausler M, Boor R, et al. Febrile infection‐related epilepsy syndrome (FIRES): a nonencephalitic encephalopathy in childhood. Epilepsia 2010;51:1323–1328. - PubMed
-
- Sakuma H, Awaya Y, Shiomi M, et al. Acute encephalitis with refractory, repetitive partial seizures (AERRPS): a peculiar form of childhood encephalitis. Acta Neurol Scand 2010;121:251–256. - PubMed
-
- Wilder‐Smith EP, Lim EC, Teoh HL, et al. The NORSE (new‐onset refractory status epilepticus) syndrome: defining a disease entity. Ann Acad Med Singapore 2005;34:417–420. - PubMed
-
- Mikaeloff Y, Jambaque I, Hertz‐Pannier L, et al. Devastating epileptic encephalopathy in school‐aged children (DESC): a pseudo encephalitis. Epilepsy Res 2006;69:67–79. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
