

Gallbladder polyps ultrasound: what the sonographer needs to know
- PMID: 33548050
- PMCID: PMC8137797
- DOI: 10.1007/s40477-021-00563-1
Gallbladder polyps ultrasound: what the sonographer needs to know
Abstract
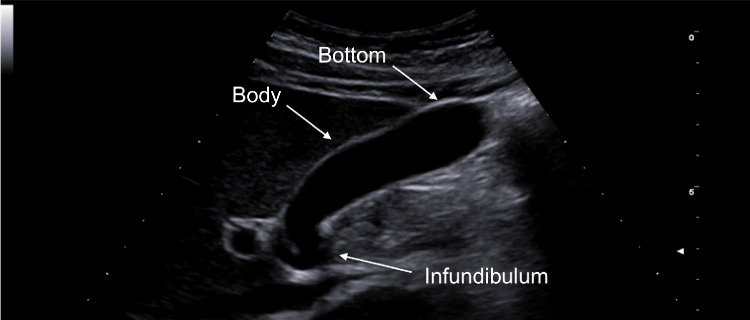
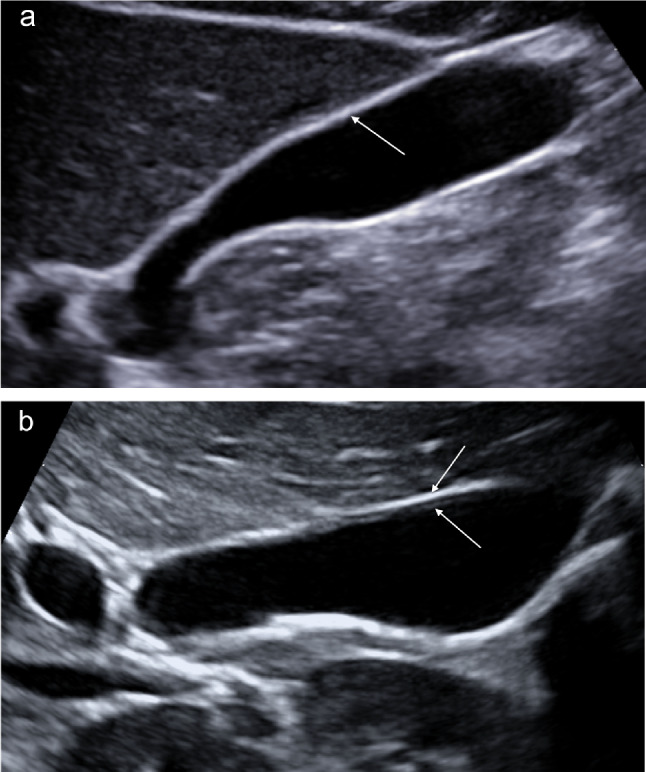
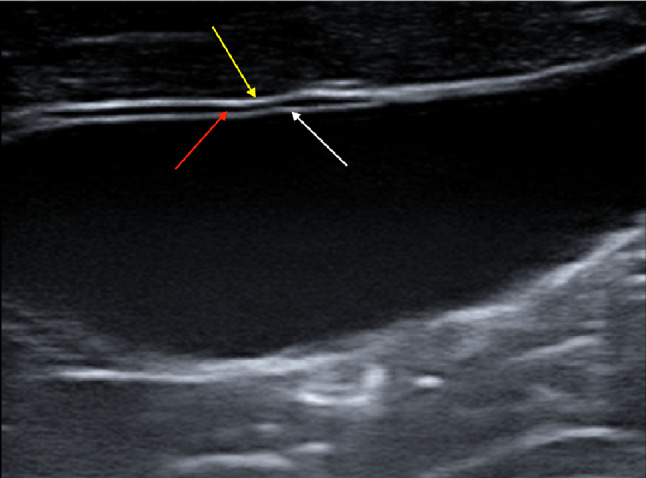
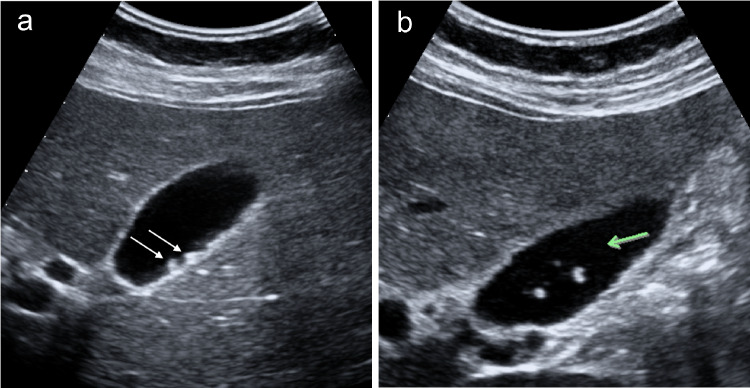
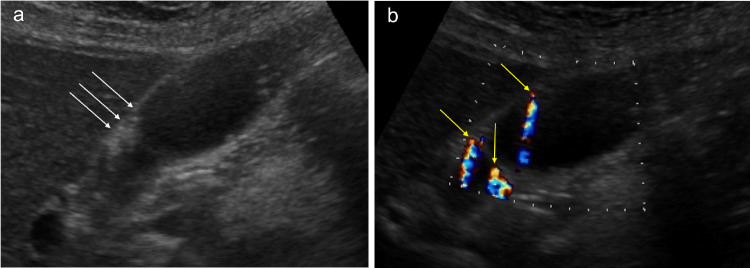
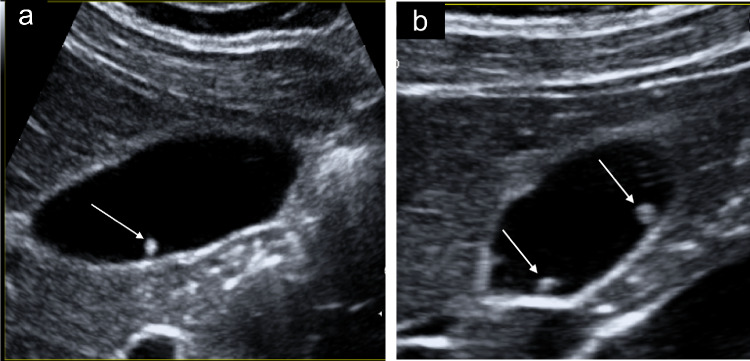
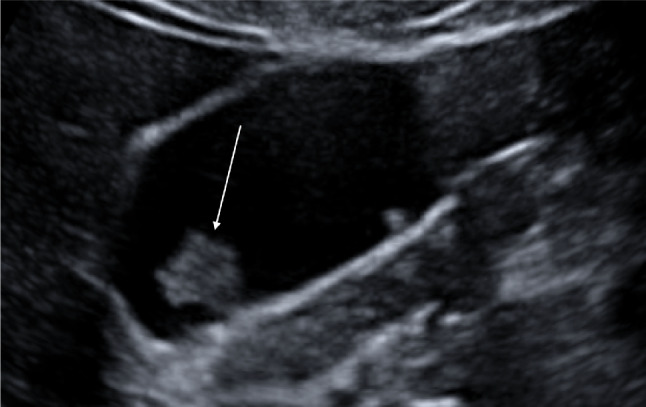
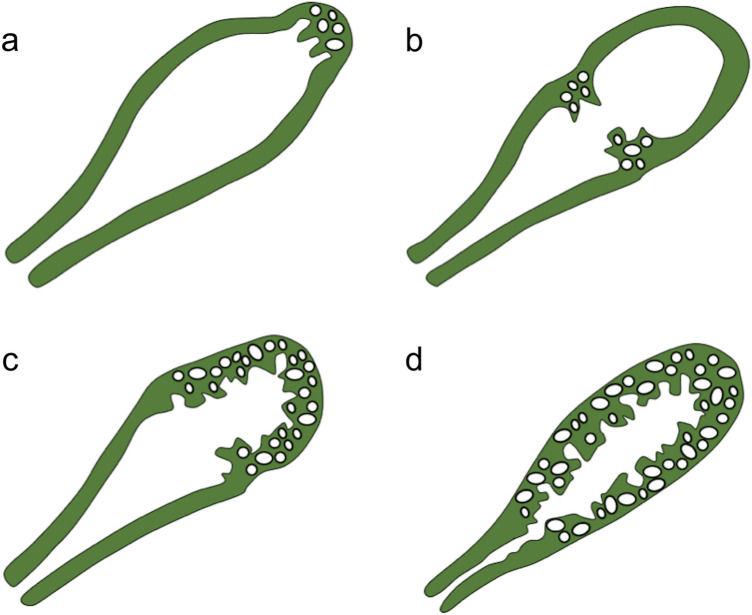
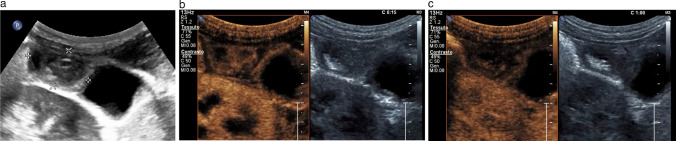
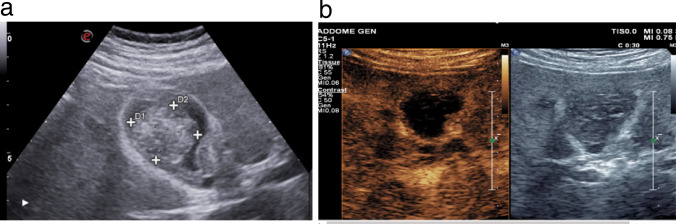
Gallbladder polyps are protuberances of the gallbladder wall projecting into the lumen. They are usually incidentally found during abdominal sonography or diagnosed on histopathology of a surgery specimen, with an estimated prevalence of up to 9.5% of patients. Gallbladder polyps are not mobile and do not demonstrate posterior acoustic shadowing; they may be sessile or pedunculated. Gallbladder polyps may be divided into pseudopolyps and true polyps. Pseudopolyps are benign and include cholesterolosis, cholesterinic polyps, inflammatory polyps, and localised adenomyomatosis. True gallbladder polyps can be benign or malignant. Benign polyps are most commonly adenomas, while malignant polyps are adenocarcinomas and metastases. There are also rare types of benign and malignant true gallbladder polyps, including mesenchymal tumours and lymphomas. Ultrasound is the first-choice imaging method for the diagnosis of gallbladder polyps, representing an indispensable tool for ensuring appropriate management. It enables limitation of secondary level investigations and avoidance of unnecessary cholecystectomies.
Keywords: Gallbladder; Polyps; Ultrasound.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
