

Do Patients With COVID-19 Benefit from Rehabilitation? Functional Outcomes of the First 100 Patients in a COVID-19 Rehabilitation Unit
- PMID: 33548208
- PMCID: PMC7857995
- DOI: 10.1016/j.apmr.2021.01.069
Do Patients With COVID-19 Benefit from Rehabilitation? Functional Outcomes of the First 100 Patients in a COVID-19 Rehabilitation Unit
Abstract
Objective: To determine the benefits associated with brief inpatient rehabilitation for coronavirus 2019 (COVID-19) patients.
Design: Retrospective chart review.
Setting: A newly created specialized rehabilitation unit in a tertiary care medical center.
Participants: Consecutive sample of patients (N=100) with COVID-19 infection admitted to rehabilitation.
Intervention: Inpatient rehabilitation for postacute care COVID-19 patients.
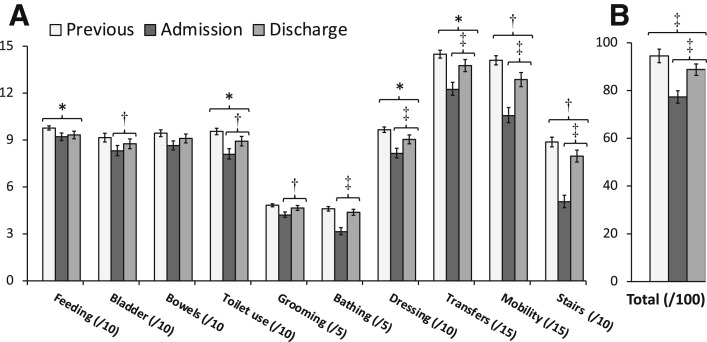
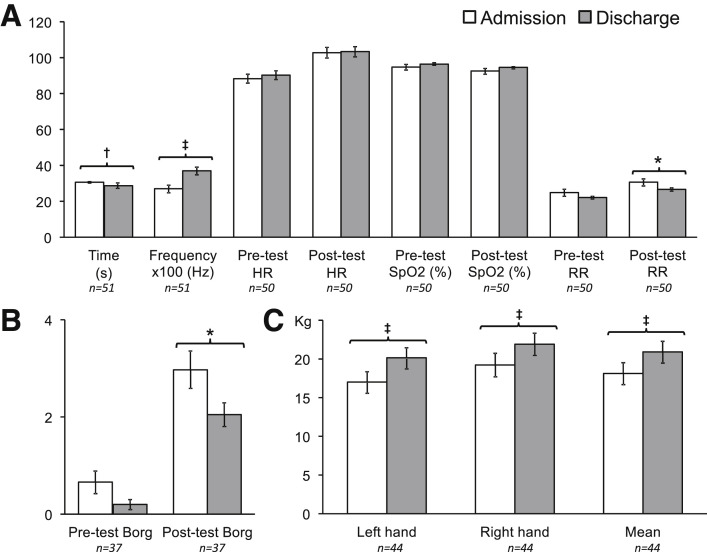
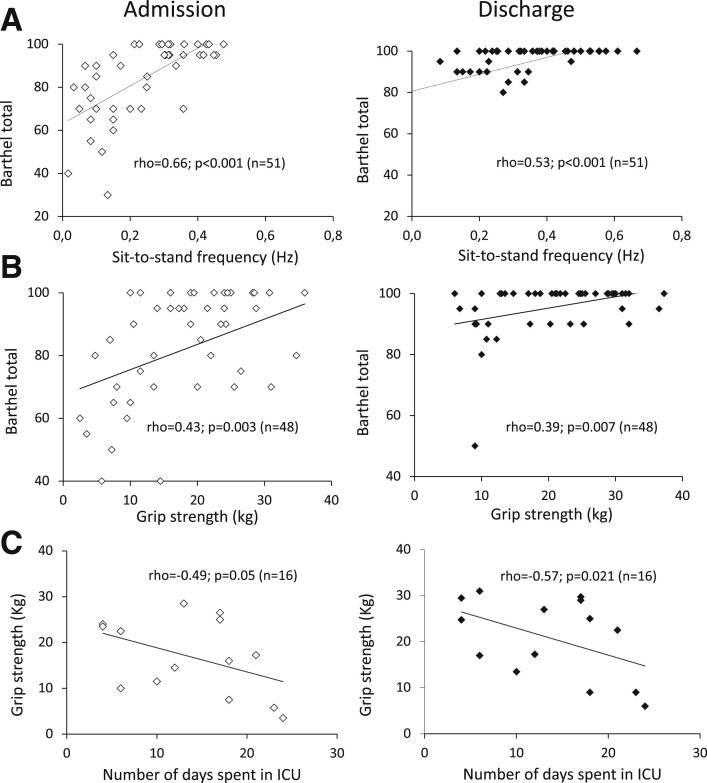
Main outcome measures: Measurements at admission and discharge comprised a Barthel Activities of Daily Living Index (including baseline value before COVID-19 infection), time to perform 10 sit-to-stands with associated cardiorespiratory changes, and grip strength (dynamometry). Correlations between these outcomes and the time spent in the intensive care unit (ICU) were explored.
Results: Upon admission to rehabilitation, 66% of the patients were men, the age was 66±22 years, mean delay from symptom onset was 20.4±10.0 days, body mass index was 26.0±5.4 kg/m2, 49% had hypertension, 29% had diabetes, and 26% had more than 50% pulmonary damage on computed tomographic scans. The mean length of rehabilitation stay was 9.8±5.6 days. From admission to discharge, the Barthel index increased from 77.3±26.7 to 88.8±24.5 (P<.001), without recovering baseline values (94.5±16.2; P<.001). There was a 37% improvement in sit-to-stand frequency (0.27±0.16 to 0.37±0.16 Hz; P<.001), a 13% decrease in post-test respiratory rate (30.7±12.6 to 26.6±6.1; P=.03), and a 15% increase in grip strength (18.1±9.2 to 20.9±8.9 kg; P<.001). At both admission and discharge, Barthel score correlated with grip strength (ρ=0.39-0.66; P<.01), which negatively correlated with time spent in the ICU (ρ=-0.57 to -0.49; P<.05).
Conclusions: Inpatient rehabilitation for COVID-19 patients was associated with substantial motor, respiratory, and functional improvement, especially in severe cases, although there remained mild persistent autonomy loss upon discharge. After acute stages, COVID-19, primarily a respiratory disease, might convert into a motor impairment correlated with the time spent in intensive care.
Keywords: COVID-19; Pandemics; Rehabilitation.
Copyright © 2021 American Congress of Rehabilitation Medicine. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Andrenelli E., Negrini F., De Sire A., et al. Rehabilitation and COVID-19: a rapid living systematic review 2020 by Cochrane Rehabilitation Field. Update as of September 30th, 2020. Eur J Phys Rehabil Med. 2020;56:846–852. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
