

Functional Dyspepsia and Gastroparesis in Tertiary Care are Interchangeable Syndromes With Common Clinical and Pathologic Features
- PMID: 33548234
- PMCID: PMC8547190
- DOI: 10.1053/j.gastro.2021.01.230
Functional Dyspepsia and Gastroparesis in Tertiary Care are Interchangeable Syndromes With Common Clinical and Pathologic Features
Abstract
Background: The aim of this study was to clarify the pathophysiology of functional dyspepsia (FD), a highly prevalent gastrointestinal syndrome, and its relationship with the better-understood syndrome of gastroparesis.
Methods: Adult patients with chronic upper gastrointestinal symptoms were followed up prospectively for 48 weeks in multi-center registry studies. Patients were classified as having gastroparesis if gastric emptying was delayed; if not, they were labeled as having FD if they met Rome III criteria. Study analysis was conducted using analysis of covariance and regression models.
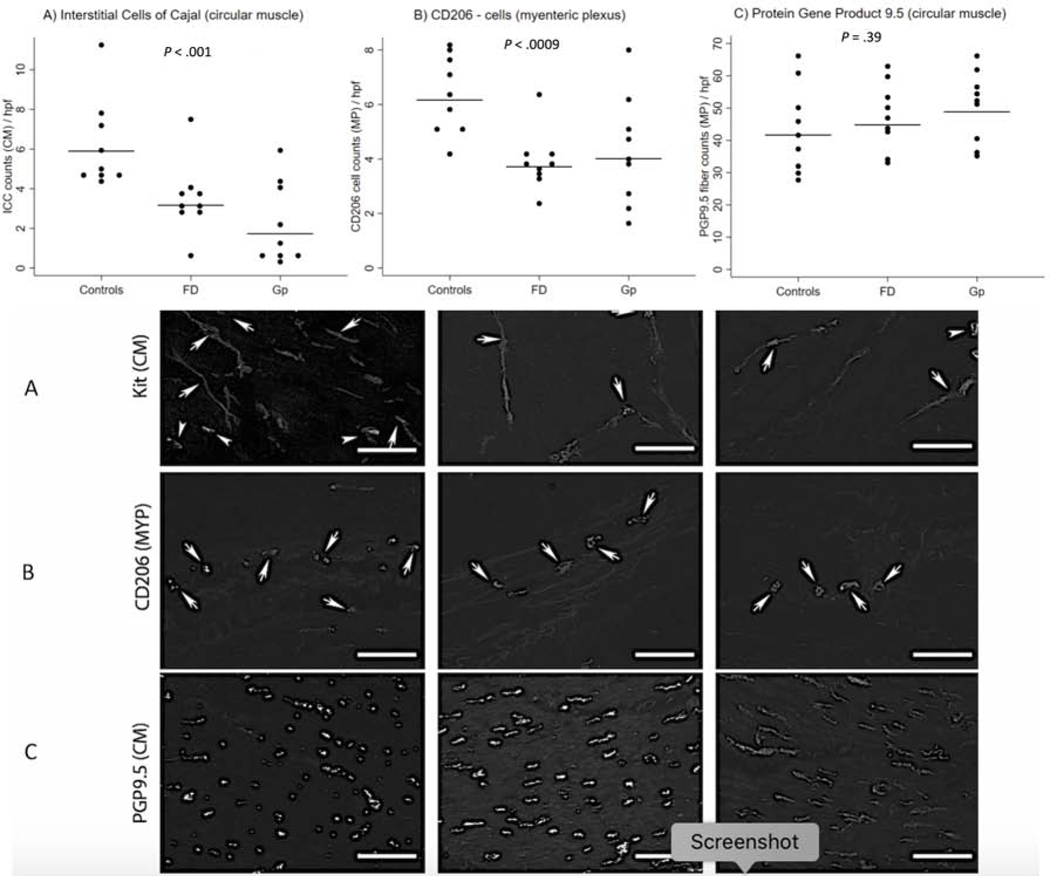
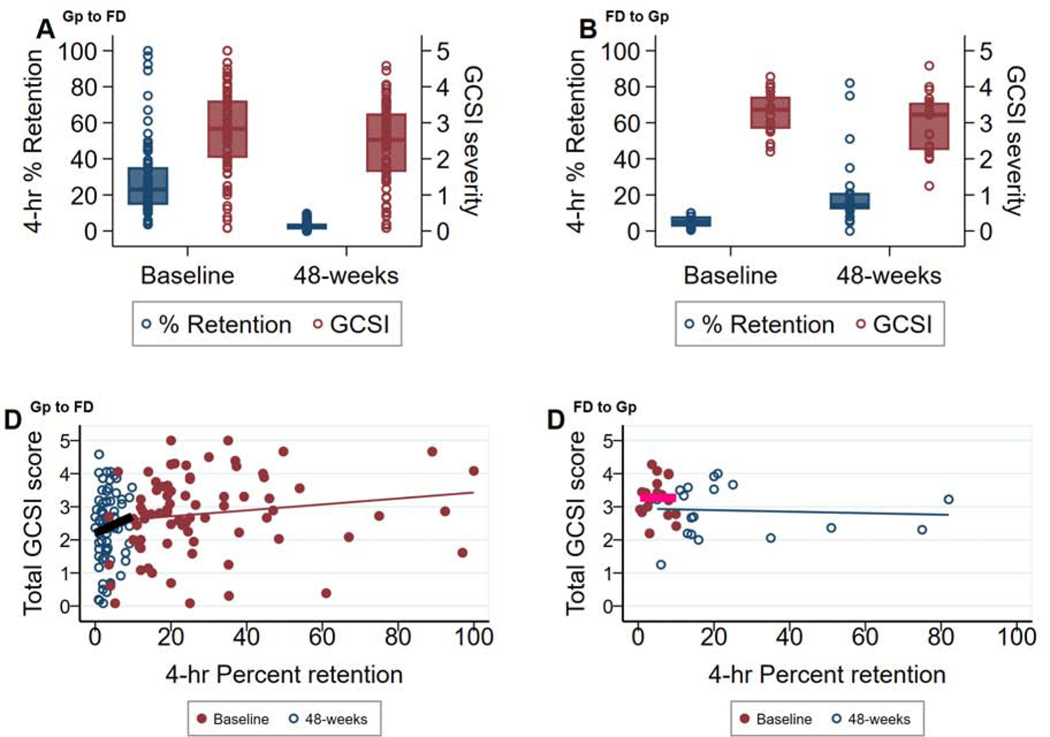
Results: Of 944 patients enrolled during a 12-year period, 720 (76%) were in the gastroparesis group and 224 (24%) in the FD group. Baseline clinical characteristics and severity of upper gastrointestinal symptoms were highly similar. The 48-week clinical outcome was also similar but at this time 42% of patients with an initial diagnosis of gastroparesis were reclassified as FD based on gastric-emptying results at this time point; conversely, 37% of patients with FD were reclassified as having gastroparesis. Change in either direction was not associated with any difference in symptom severity changes. Full-thickness biopsies of the stomach showed loss of interstitial cells of Cajal and CD206+ macrophages in both groups compared with obese controls.
Conclusions: A year after initial classification, patients with FD and gastroparesis, as seen in tertiary referral centers at least, are not distinguishable based on clinical and pathologic features or based on assessment of gastric emptying. Gastric-emptying results are labile and do not reliably capture the pathophysiology of clinical symptoms in either condition. FD and gastroparesis are unified by characteristic pathologic features and should be considered as part of the same spectrum of truly "organic" gastric neuromuscular disorders. CLINICALTRIALS.
Gov identifier: NCT00398801, NCT01696747.
Keywords: Chronic Nausea; Enteric Nervous System; Functional Dyspepsia; Gastric Emptying; Gastroparesis.
Copyright © 2021 AGA Institute. All rights reserved.
Conflict of interest statement
Conflict of Interest
The authors declare that there is no conflict of interests in this study.
Figures
Comment in
-
Gastroparesis: A Dead-end Street After All?Gastroenterology. 2021 May;160(6):1931-1933. doi: 10.1053/j.gastro.2021.02.042. Epub 2021 Feb 20. Gastroenterology. 2021. PMID: 33621562 No abstract available.
-
Is the Quantification of Interstitial Cells of Cajal in Gastric Biopsy Samples in Patients With Gastroparesis Ready for Prime Time?Gastroenterology. 2023 Jul;165(1):1-4. doi: 10.1053/j.gastro.2023.03.204. Epub 2023 Mar 16. Gastroenterology. 2023. PMID: 36933624 Free PMC article. No abstract available.
References
-
- Abell TL, Bernstein RK, Cutts T, et al. Treatment of gastroparesis: a multidisciplinary clinical review. Neurogastroenterol Motil 2006;18:263–83. - PubMed
-
- Talley NJ, Holtmann G. Irritable bowel syndrome and functional dyspepsia: what can epidemiology tell us about etiology? Expert Rev Gastroenterol Hepatol 2018;12:633–5. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- U24 DK074008/DK/NIDDK NIH HHS/United States
- U01 DK074008/DK/NIDDK NIH HHS/United States
- U01 DK112194/DK/NIDDK NIH HHS/United States
- U01 DK074007/DK/NIDDK NIH HHS/United States
- U01 DK073975/DK/NIDDK NIH HHS/United States
- U01 DK074035/DK/NIDDK NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- U01 DK073974/DK/NIDDK NIH HHS/United States
- UL1 TR003098/TR/NCATS NIH HHS/United States
- U01 DK073983/DK/NIDDK NIH HHS/United States
- UL1 TR000135/TR/NCATS NIH HHS/United States
- U01 DK112193/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
