

Arterial Thrombotic Events in Adult Inpatients With COVID-19
- PMID: 33549252
- PMCID: PMC7691140
- DOI: 10.1016/j.mayocp.2020.11.018
Arterial Thrombotic Events in Adult Inpatients With COVID-19
Abstract
Objective: To evaluate the clinical course of and risk factors for arterial thrombotic events in adult inpatients with coronavirus disease 2019 (COVID-19).
Methods: All consecutive adult patients admitted for COVID-19 infection in a referral center in France and discharged from the hospital between April 1 and April 30, 2020, were included. All arterial thrombotic events that occurred through discharge were considered for analysis. Epidemiologic, demographic, clinical, laboratory, treatment, and outcome data were extracted from electronic medical records with use of a standardized data collection form.
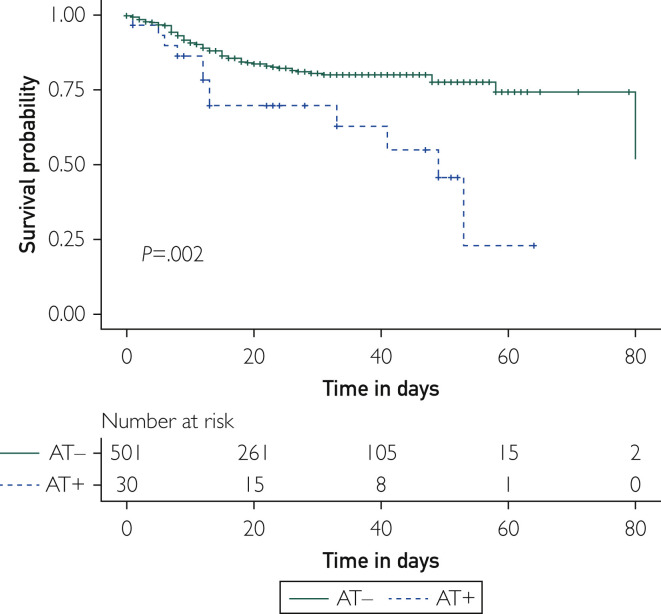
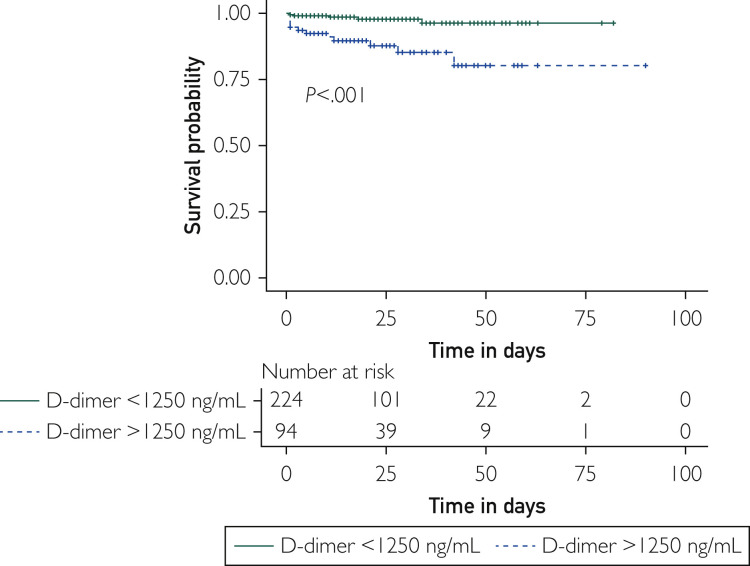
Results: Overall, 531 COVID-19+ patients were analyzed. Among them, 30 (5.6%) experienced arterial thrombotic events. Arterial thrombotic events in the setting of COVID-19 infection happened at a median of 11 (5-20) days after the first symptoms of infection; occurred in high-risk patients according to traditional cardiovascular risk factors; had an atypical pattern, such as thrombosis of the aorta, upper limb, or renal arteries or cerebral microvasculopathy in 7 (23.3%) cases; and were associated with an in-hospital mortality rate of 40%. Arterial thrombotic events increased the risk of death by 3-fold in COVID-19+ patients (hazard ratio, 2.96; 95% CI, 1.4 to 4.7; P=.002). A subdistribution survival hazard model showed that a concentration of D-dimer above 1250 ng/mL increased the risk of arterial thrombotic events in COVID-19+ patients by more than 7 (subdistribution hazard ratio, 7.68; 95% CI, 2.9 to 20.6; P<.001).
Conclusion: A dramatically high rate of in-hospital death was observed in patients who suffered arterial thrombotic events in the setting of COVID-19 infection. A D-dimer level above 1250 ng/mL at entry may identify COVID-19+ patients at risk for arterial thrombotic events.
Copyright © 2020 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
