

Effect of variable pre-oxygenation endpoints on safe apnoea time using high flow nasal oxygen for women in labour: a modelling investigation
- PMID: 33549319
- PMCID: PMC8132878
- DOI: 10.1016/j.bja.2020.12.031
Effect of variable pre-oxygenation endpoints on safe apnoea time using high flow nasal oxygen for women in labour: a modelling investigation
Abstract
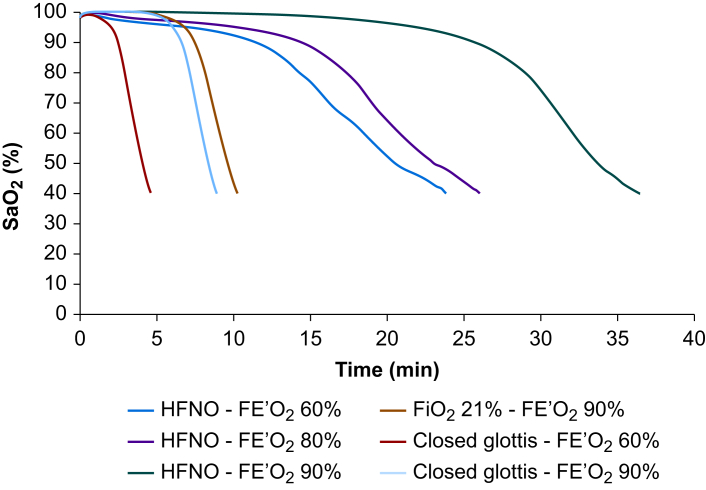
Background: Studies of pulmonary denitrogenation (pre-oxygenation) in obstetric populations have shown high flow nasal oxygen therapy (HFNO) is inferior to facemask techniques. HFNO achieves median end-tidal oxygen fraction (FE'O2) of 0.87 after 3 min. As HFNO prolongs safe apnoea times through apnoeic oxygenation, we postulated that HFNO would still extend safe apnoeic times despite the lower FE'O2 after pre-oxygenation.
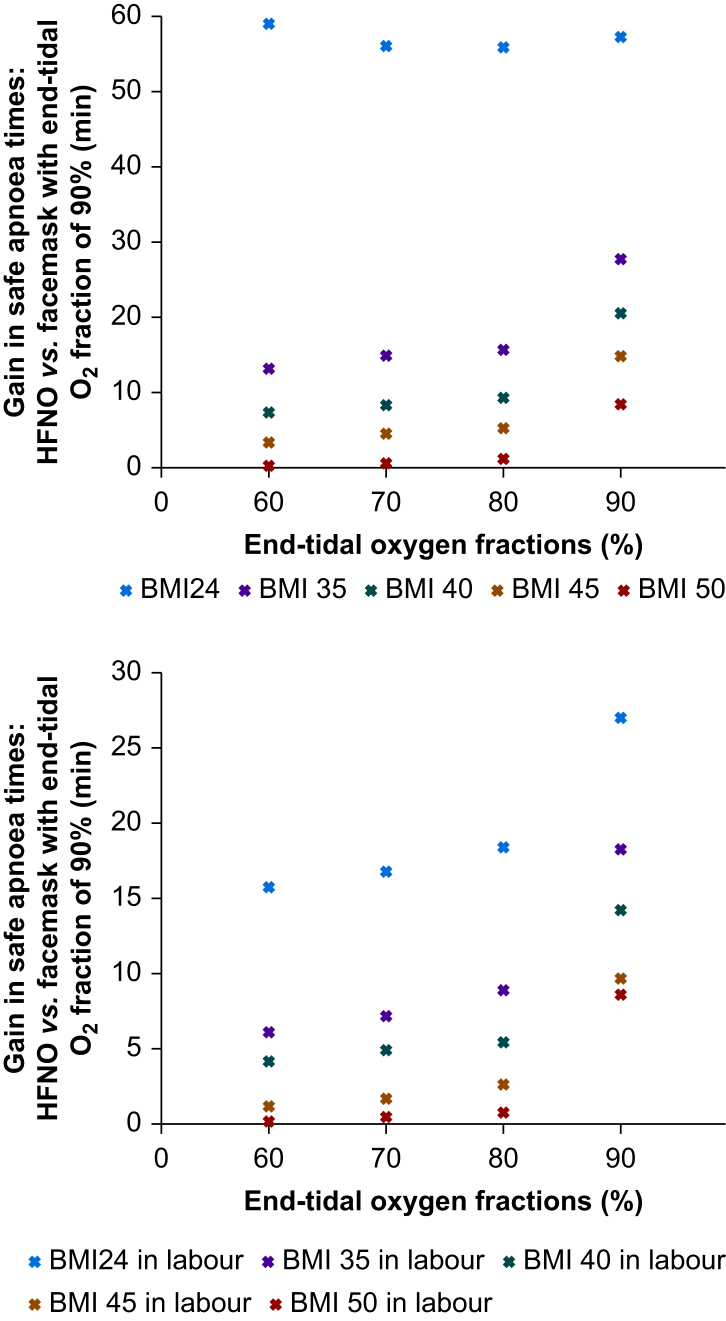
Methods: The Interdisciplinary Collaboration in Systems Medicine simulation suite, a highly integrated, high-fidelity model of the human respiratory and cardiovascular systems, was used to study the effect of varying FE'O2 (60%, 70%, 80%, and 90%) on the duration of safe apnoea times using HFNO and facemask techniques (with the airway open and obstructed). The study population consisted of validated models of pregnant women in active labour and not in labour with BMI of 24, 35, 40, 45, and 50 kg m-2.
Results: HFNO provided longer safe apnoeic times in all models, with all FE'O2 values. Labour and increased BMI reduced this effect, in particular a BMI of 50 kg m-2 reduced the improvement in apnoea time to 1.8-8.5 min (depending on the FE'O2), compared with an improvement of more than 60 min in the subject with BMI 24 kg m-2.
Conclusions: Despite generating lower FE'O2, HFNO provides longer safe apnoea times in pregnant subjects in labour. Care should be taken when used in patients with BMI ≥50 kg m-2 as the extension of the safe apnoea time is limited.
Keywords: apnoea; computer simulation; high-flow nasal oxygenation; obesity in pregnancy; obstetrics.
Copyright © 2021 British Journal of Anaesthesia. Published by Elsevier Ltd. All rights reserved.
Figures
Similar articles
-
Comparison of apnoeic oxygen techniques in term pregnant subjects: a computational modelling study.Br J Anaesth. 2022 Oct;129(4):581-587. doi: 10.1016/j.bja.2022.06.021. Epub 2022 Aug 11. Br J Anaesth. 2022. PMID: 35963819
-
The effect of transnasal humidified rapid-insufflation ventilator exchange (THRIVE) versus nasal prongs on safe apnoea time in paralysed obese patients: a randomised controlled trial.Br J Anaesth. 2022 Feb;128(2):375-381. doi: 10.1016/j.bja.2021.10.048. Epub 2021 Dec 8. Br J Anaesth. 2022. PMID: 34895717 Clinical Trial.
-
Pre-oxygenation using high flow humidified nasal oxygen or face mask oxygen in pregnant people - a prospective randomised controlled crossover non-inferiority study (The HINOP2 study).Int J Obstet Anesth. 2024 Nov;60:104236. doi: 10.1016/j.ijoa.2024.104236. Epub 2024 Jul 23. Int J Obstet Anesth. 2024. PMID: 39209574 Clinical Trial.
-
Comparison of the effectiveness of high-flow nasal oxygen vs. standard facemask oxygenation for pre- and apneic oxygenation during anesthesia induction: a systematic review and meta-analysis.BMC Anesthesiol. 2022 Apr 6;22(1):100. doi: 10.1186/s12871-022-01615-7. BMC Anesthesiol. 2022. PMID: 35387583 Free PMC article.
-
Effectiveness of preoxygenation strategies: a systematic review and network meta-analysis.Br J Anaesth. 2024 Jul;133(1):152-163. doi: 10.1016/j.bja.2024.02.028. Epub 2024 Apr 9. Br J Anaesth. 2024. PMID: 38599916
Cited by
-
Supreme laryngeal mask airway for cesarean section under general anesthesia: a 10-year retrospective cohort study.Front Med (Lausanne). 2023 Jul 20;10:1181503. doi: 10.3389/fmed.2023.1181503. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37547618 Free PMC article.
-
Pre-oxygenation with high-flow oxygen through the nasopharyngeal airway compared to facemask on carbon dioxide clearance in emergency adults: a prospective randomized non-blinded clinical trial.Eur J Trauma Emerg Surg. 2024 Jun;50(3):1051-1061. doi: 10.1007/s00068-023-02418-2. Epub 2023 Dec 26. Eur J Trauma Emerg Surg. 2024. PMID: 38148421 Free PMC article. Clinical Trial.
-
Apnoeic oxygenation in morbid obesity: a randomised controlled trial comparing facemask and high-flow nasal oxygen delivery.Br J Anaesth. 2023 Jan;130(1):103-110. doi: 10.1016/j.bja.2021.12.011. Epub 2022 Jan 11. Br J Anaesth. 2023. PMID: 35027169 Free PMC article. Clinical Trial.
References
-
- Porter R., Wrench I.J., Freeman R. Preoxygenation for general anaesthesia in pregnancy: is it adequate? Int J Obstet Anesth. 2011;20:363–365. - PubMed
-
- Douglas M.J., Preston R.L. The obstetric airway: things are seldom as they seem. Can J Anesth. 2011;58:494. - PubMed
-
- Doyle A.J., Stolady D., Mariyaselvam M. Preoxygenation and apneic oxygenation using transnasal humidified rapid-insufflation ventilatory exchange for emergency intubation. J Crit Care. 2016;36:8–12. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
