

Ultra-Small Lung Cysts Impair Diffusion Without Obstructing Air Flow in Lymphangioleiomyomatosis
- PMID: 33549601
- PMCID: PMC8295912
- DOI: 10.1016/j.chest.2021.01.077
Ultra-Small Lung Cysts Impair Diffusion Without Obstructing Air Flow in Lymphangioleiomyomatosis
Abstract
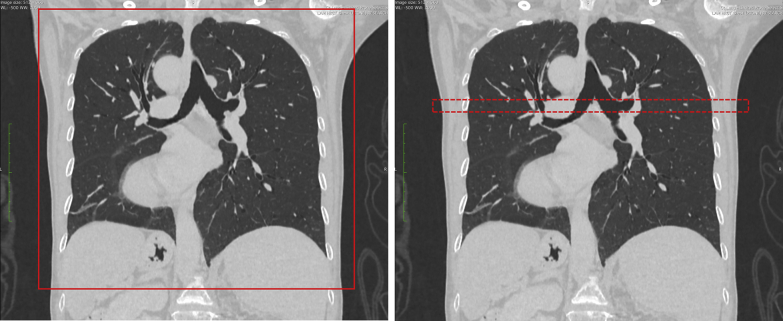
Background: Lymphangioleiomyomatosis (LAM) is a rare lung disease found primarily in women of childbearing age, characterized by the formation of air-filled cysts, which may be associated with reductions in lung function. An experimental, regional ultra-high resolution CT scan identified an additional volume of cysts relative to standard chest CT imaging, which consisted primarily of ultra-small cysts.
Research question: What is the impact of these ultra-small cysts on the pulmonary function of patients with LAM?
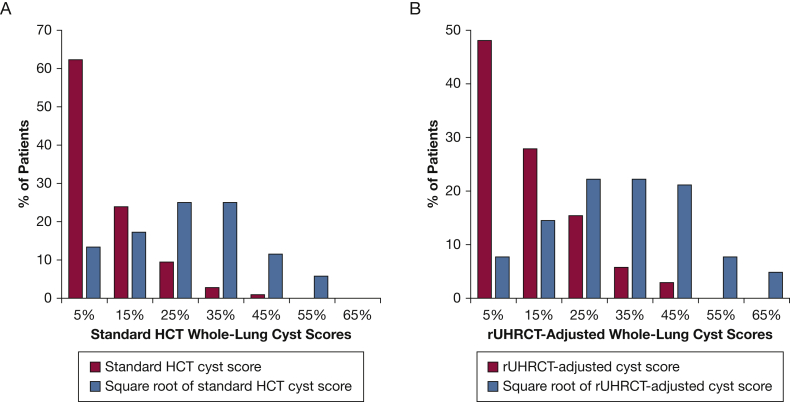
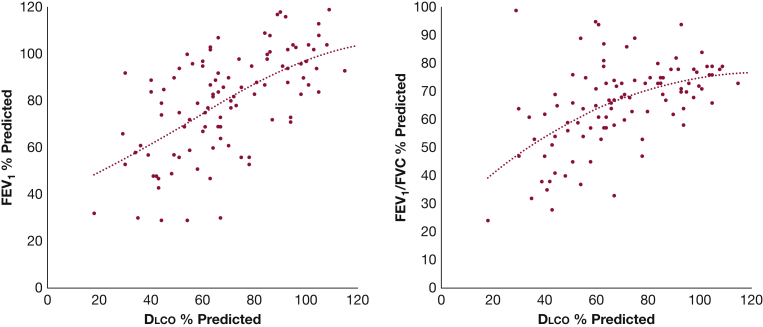
Study design and methods: A group of 103 patients with LAM received pulmonary function tests and a CT examination in the same visit. Cyst score, the percentage lung volume occupied by cysts, was measured by using commercial software approved by the US Food and Drug Administration. The association between cyst scores and pulmonary function tests of diffusing capacity of the lungs for carbon monoxide (Dlco) (% predicted), FEV1 (% predicted), and FEV1/FVC (% predicted) was assessed with statistical analysis adjusted for demographic variables. The distributions of average cyst size and ultra-small cyst fraction among the patients were evaluated.
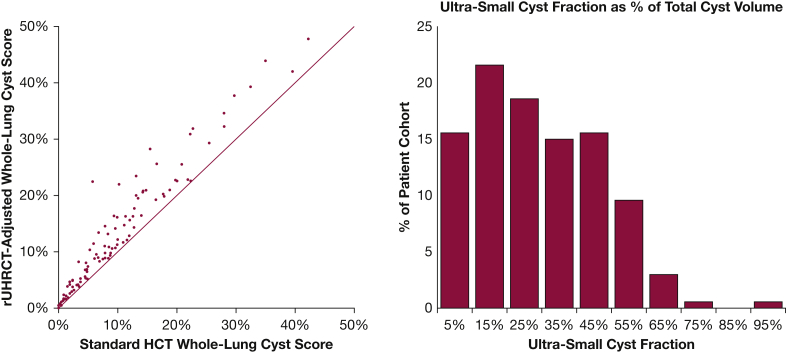
Results: The additional cyst volume identified by the experimental, higher resolution scan consisted of cysts of 2.2 ± 0.8 mm diameter on average and are thus labeled the "ultra-small cyst fraction." It accounted for 27.9 ± 19.0% of the total cyst volume among the patients. The resulting adjusted, whole-lung cyst scores better explained the variance of Dlco (P < .001 adjusted for multiple comparisons) but not FEV1 and FEV1/FVC (P = 1.00). The ultra-small cyst fraction contributed to the reduction in Dlco (P < .001) but not to FEV1 and FEV1/FVC (P = .760 and .575, respectively). The ultra-small cyst fraction and average cyst size were correlated with cyst burden, FEV1, and FEV1/FVC but less with Dlco.
Interpretation: The ultra-small cysts primarily contributed to the reduction in Dlco, with minimal effects on FEV1 and FEV1/FVC. Patients with lower cyst burden and better FEV1 and FEV1/FVC tended to have smaller average cyst size and higher ultra-small cyst fraction.
Clinical trial registration: ClinicalTrials.gov; No.: NCT00001465; URL: www.clinicaltrials.gov.
Published by Elsevier Inc.
Figures



References
-
- Hohman D.W., Noghrehkar D., Ratnayake S. Lymphangioleiomyomatosis: a review. Eur J Intern Med. 2008;19(5):319–324. - PubMed
-
- Harknett E.C., Chang W.Y.C., Byrnes S. Use of variability in national and regional data to estimate the prevalence of lymphangioleiomyomatosis. QJM Int J Med. 2011;104(11):971–979. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
