

Endoscopic Phenotype of the J Pouch in Patients With Inflammatory Bowel Disease: A New Classification for Pouch Outcomes
- PMID: 33549868
- PMCID: PMC8339185
- DOI: 10.1016/j.cgh.2021.02.010
Endoscopic Phenotype of the J Pouch in Patients With Inflammatory Bowel Disease: A New Classification for Pouch Outcomes
Abstract
Background & aims: Pouchitis is a common complication of ileal pouch-anal anastomosis (IPAA) in patients with ulcerative colitis who have undergone colectomy. Pouchitis has been considered a single entity despite a broad array of clinical and endoscopic patterns. We developed a novel classification system based on the pattern of inflammation observed in pouches and evaluated the contributing factors and prognosis of each phenotype.
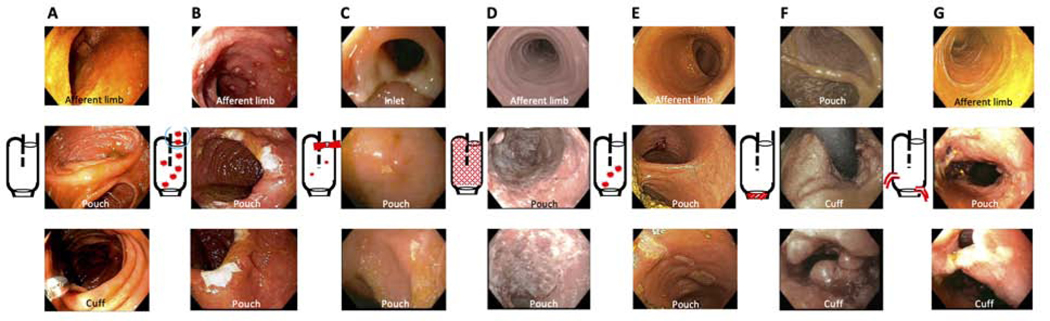
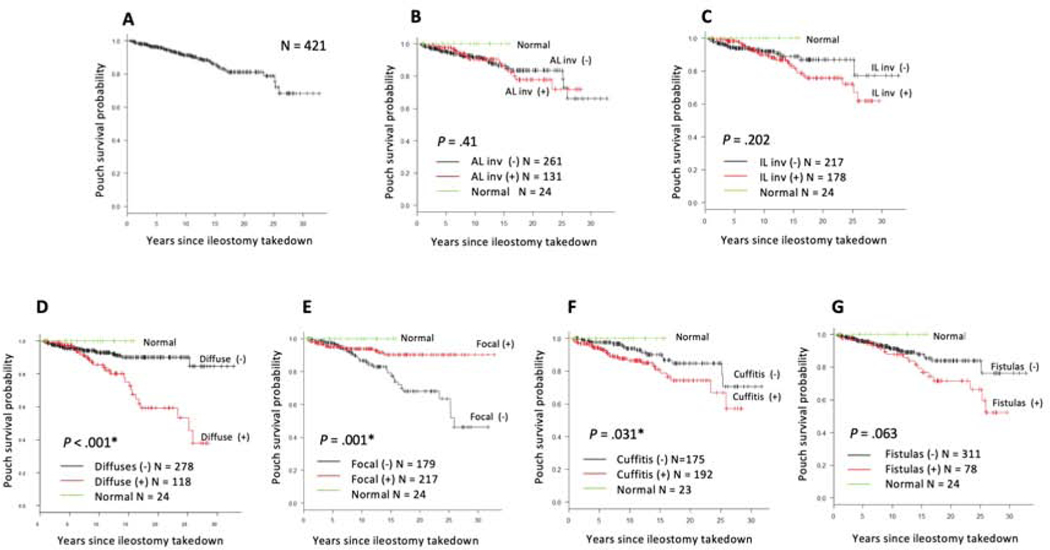
Methods: We identified 426 patients (384 with ulcerative colitis) treated with proctocolectomy and IPAA who subsequently underwent pouchoscopies at the University of Chicago between June 1997 and December 2019. We retrospectively reviewed 1359 pouchoscopies and classified them into 7 main pouch phenotypes: (1) normal, (2) afferent limb involvement, (3) inlet involvement, (4) diffuse, (5) focal inflammation of the pouch body, (6) cuffitis, and (7) pouch with fistulas noted 6 months after ileostomy takedown. Logistic regression analysis was used to assess factors contributing to each phenotype. Pouch survival was estimated by the log-rank test and the Cox proportional hazards model.
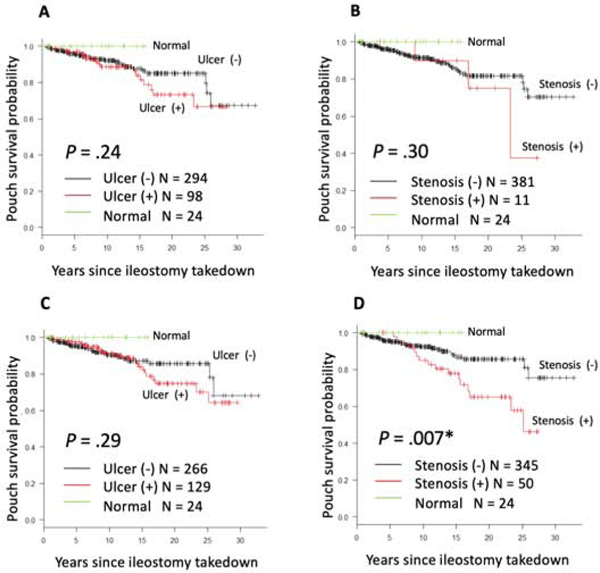
Results: Significant contributing factors for afferent limb involvement were a body mass index of 25 or higher and hand-sewn anastomosis, for inlet involvement the significant contributing factor was male sex; for diffuse inflammation the significant contributing factors were extensive colitis and preoperative use of anti-tumor necrosis factor drugs, for cuffitis the significant contributing factors were stapled anastomosis and preoperative Clostridioides difficile infection. Inlet stenosis, diffuse inflammation, and cuffitis significantly increased the risk of pouch excision. Diffuse inflammation was associated independently with pouch excision (hazard ratio, 2.69; 95% CI, 1.34-5.41; P = .005).
Conclusions: We describe 7 unique IPAA phenotypes with different contributing factors and outcomes, and propose a new classification system for pouch management and future interventional studies.
Keywords: Endoscopic Phenotype; Ileal Pouch–Anal Anastomosis; Inflammatory Bowel Disease; Pouch Prognosis; Pouchitis.
Copyright © 2022 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
The Chicago Classification of Pouchitis: An Important Step Toward a Needed Consensus.Clin Gastroenterol Hepatol. 2022 Feb;20(2):281-282. doi: 10.1016/j.cgh.2021.03.025. Epub 2021 Mar 19. Clin Gastroenterol Hepatol. 2022. PMID: 33753242 No abstract available.
References
-
- Fazio VW, Kiran RP, Remzi FH, et al. Ileal pouch anal anastomosis: analysis of outcome and quality of life in 3707 patients. Ann Surg 2013;257:679–685. - PubMed
-
- Lightner AL, Mathis KL, Dozois EJ, et al. Results at Up to 30 Years After Ileal Pouch-Anal Anastomosis for Chronic Ulcerative Colitis. Inflamm Bowel Dis 2017;23:781–790. - PubMed
-
- Sandborn WJ, Tremaine WJ, Batts KP, et al. Pouchitis after ileal pouch-anal anastomosis: a Pouchitis Disease Activity Index. Mayo Clin Proc 1994;69:409–415. - PubMed
-
- Manilich E, Remzi FH, Fazio VW, et al. Prognostic modeling of preoperative risk factors of pouch failure. Dis Colon Rectum 2012;55:393–399. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
